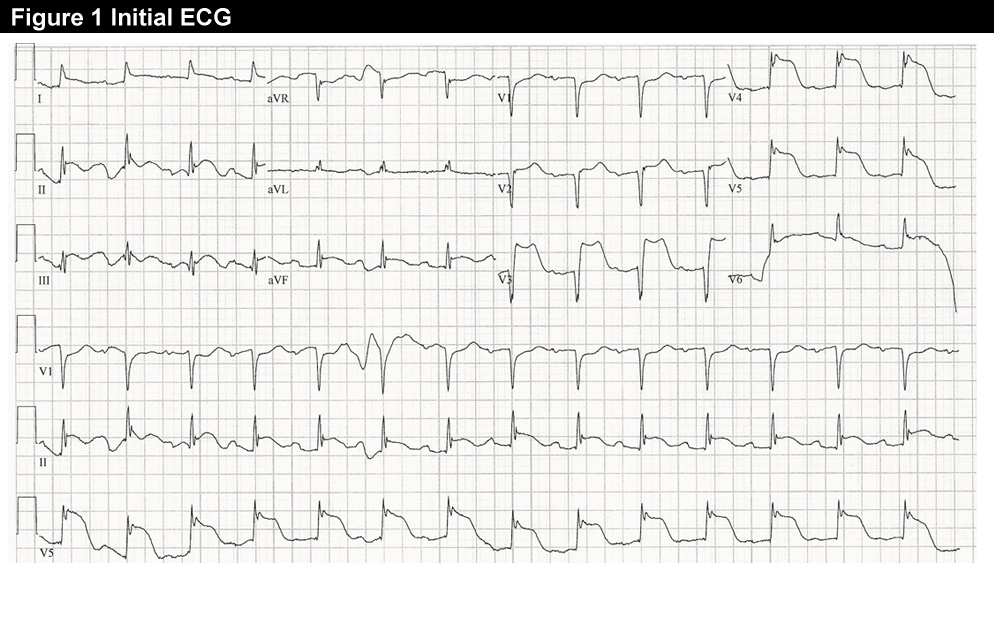
A 55-year-old male presented after having two hours of continuous, severe, substernal chest pain with associated nausea, vomiting and left arm radiation. The initial ECG showed anterior ST-elevation V1-V6 (Figure 1). He underwent emergent PCI. Thrombectomy was used, with subsequent stenting with TIMI grade 1-2 flow. With additional treatment, TIMI flow had increased to TIMI grade 2-3 by the end of the procedure, and he was admitted to the CICU.
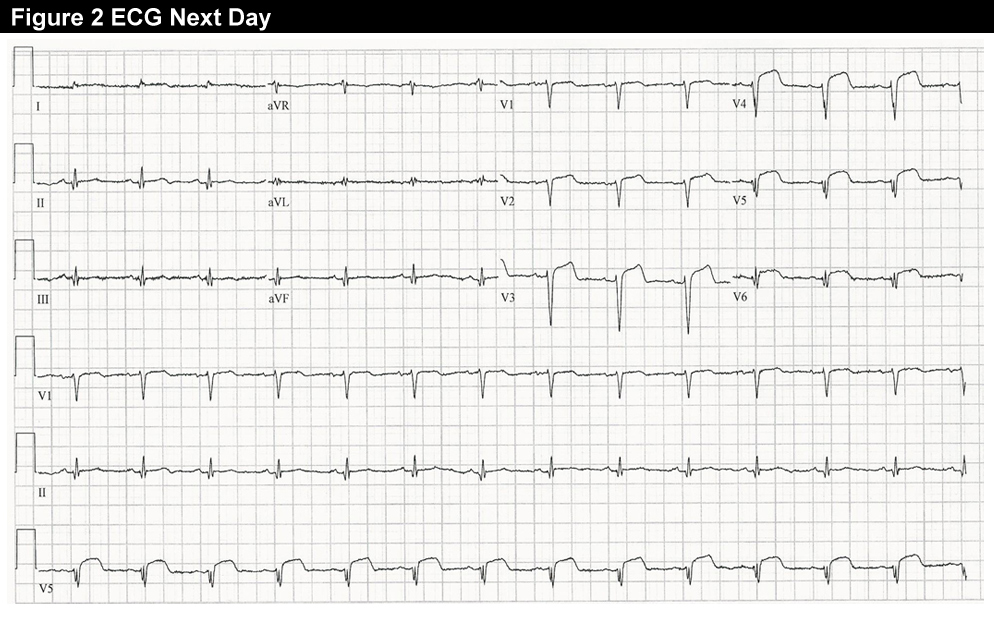
An ECG the next morning showed reduced but persistent ST elevation in V1-V3, with Q waves in V1-V6 (Figure 2).
Echocardiogram showed severe septal, anterior and apical hypokinesis to akinesis.
Four days later, he developed mild to moderate, burning indigestional upper epigastric pain, different from his presenting symptoms. The repeat ECG showed no significant change from the second day ECG (Figure 2), with persistent Q waves. The repeat echocardiogram was unchanged from prior, with no pericardial effusion.
Repeat markers were sent; the demonstrated an TnI of 8.4 ng/ml and CK-MB of 3.2 ng/ml.
What would be your next step?
Show Answer
The correct answer is: 3. Repeat TnI and MB in 2-3 hours to determine the time course of marker elevations.
After MI, Tn typically peaks within 12-24 hours, depending on the type and size of MI, and whether there is successful reperfusion.1 Earlier peaking of markers is usually associated with more successful reperfusion.
A common misconception is that troponin is primarily cleared renally. In fact, Although levels can be detected in the bloodstream for days after an MI—with the duration in part dependent on the size of the MI1,2—the serum half-life of Tn is relatively short, in hours.1
The prolonged elevations in the blood stream after MI likely reflect release from the sarcomeres with ongoing cellular necrosis.3 As levels decrease, there may be some variation in Tn levels detected, such that it is not a constant linear decrease.2 In some cases, after large MIs, serial assessment of Tn may show minor rises and falls.2
In contrast, CK-MB returns to normal values much faster, and within two to three days has fallen below the upper limit of normal.2
There is limited comparative data on the use of Tn and CK-MB for detecting reinfarction. One small study has shown that Tn and CK-MB are comparable, but this included only nine patients, and peak TnI values were relatively low, and not comparable to what would typically be seen after a STEMI.4
This may be one situation in which CK-MB offers some advantages, as it much more rapidly returns to normal after MI. In the setting of reinfarction, particularly after stent thrombosis, elevations would be well above the standard cut point, making it easier to determine if this had occurred. However, there is only limited data currently available assessing the role of Tn for reinfarction, particularly if early after STEMI.
References
Jaffe AS, Landt Y, Parvin CA, Abendschein DR, Geltman EM, Ladenson JH. Comparative sensitivity of cardiac troponin I and lactate dehydrogenase isoenzymes for diagnosing acute myocardial infarction. Clin Chem 1996;42:1770-6.
Katus HA, Remppis A, Neumann FJ, Scheffold T, Diederich KW, Vinar G, Noe A, Matern G, Kuebler W. Diagnostic efficiency of troponin T measurements in acute myocardial infarction. Circulation 1991;83:902-12.
Katus HA, Remppis A, Scheffold T, Diederich KW, Kuebler W. Intracellular compartmentation of cardiac troponin T and its release kinetics in patients with reperfused and nonreperfused myocardial infarction. Am J Cardiol 1991;67:1360-7.
Apple FS, Murakami MM. Cardiac troponin and creatine kinase MB monitoring during in-hospital myocardial reinfarction. Clin Chem 2005;51:460-3.