A 72-year-old female patient presents with a 2-month history of increasing shortness of breath and orthopnea. She is unable to walk for than a few steps before becoming dyspneic. Her comorbidities include moderate chronic obstructive pulmonary disease, asymptomatic 70% carotid stenosis, and severe rheumatoid arthritis involving the bilateral knees and hips that results in limited mobility and requires the patient to use a cane to ambulate. Physical examination reveals a 3/6 holosystolic murmur at the apex with an early diastolic filling sound and an accentuated pulmonic component of the second heart sound. A transthoracic and transesophageal echocardiogram are performed (Figure 1) that demonstrate severe mitral regurgitation (MR) due to a flail A2 segment of the mitral valve and an ejection fraction of 70%. On frailty evaluation, the patient meets two of the four criteria (reduced grip strength and 5 meter walk speed). The Society of Thoracic Surgeons risk score is 6% for mitral valve repair and 7% for replacement.
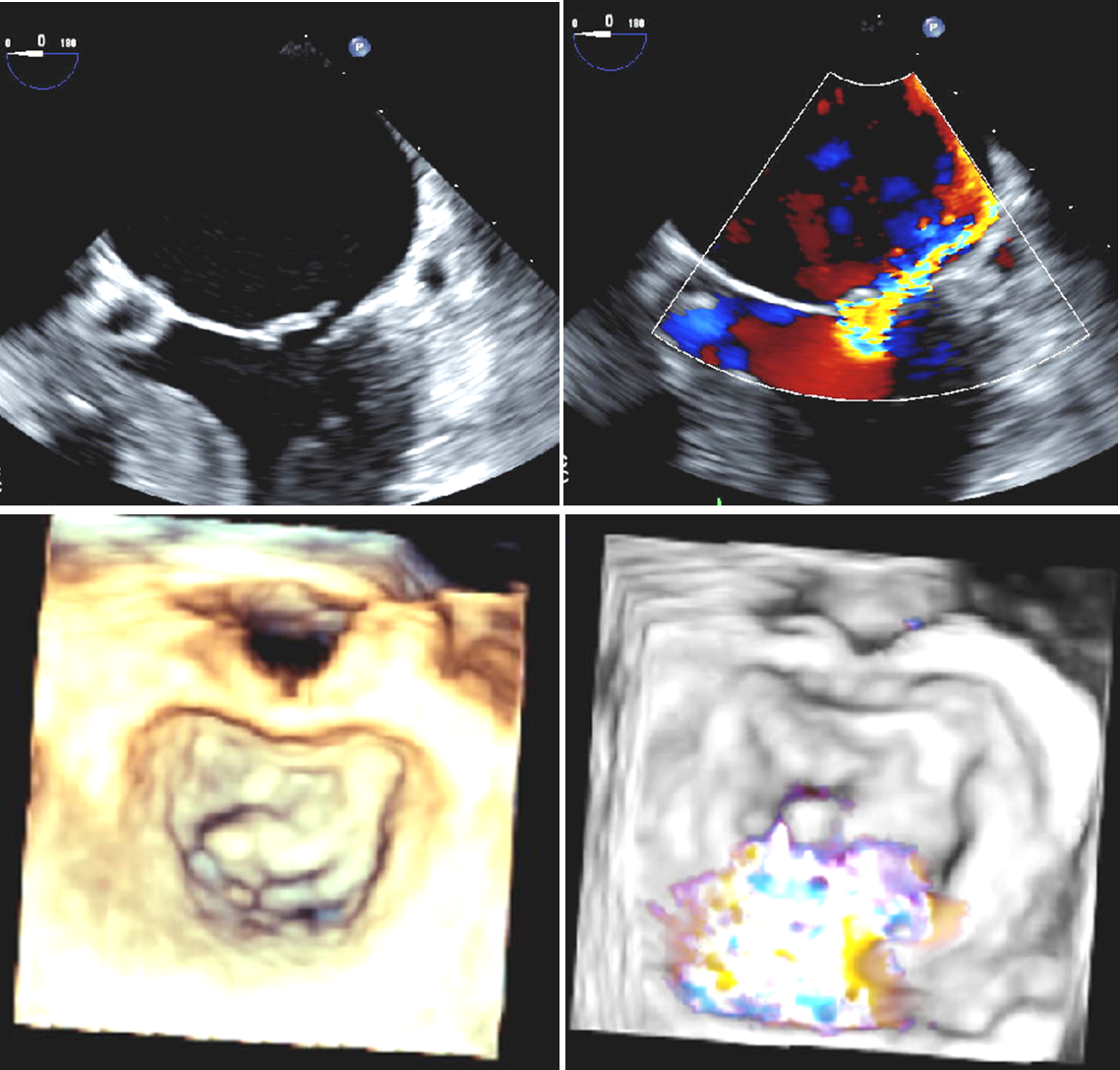
Figure 1
The top two images show a two-dimensional transesophageal echocardiogram demonstrating a flail A2 segment with resulting severe mitral valve regurgitation. The bottom two images show a three-dimensional transesophageal echocardiogram demonstrating a flail A2 segment of the mitral valve with corresponding central jet of MR.
Which of the following statements is correct regarding treatment of this patient's mitral valve regurgitation?
Show Answer
The correct answer is: D. The mitral valve anatomy of this patient is suitable for transcatheter edge-to-edge mitral valve repair.
A2/P2 pathology is associated with favorable outcomes with transcatheter mitral valve repair.1 In the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapies registry, A2/P2 pathology was associated with a higher rate of procedural success compared with a non-central location of MR.1 This patient has severe symptoms due to primary MR and is considered high risk for mitral valve surgery with two out of four frailty criteria, making transcatheter mitral valve repair the preferred treatment strategy.2
Transcatheter mitral valve replacement is still an investigational treatment primarily being studied in secondary MR and would not be suitable for this patient with primary MR. Surgical mitral valve replacement is not the preferred approach in a patient with mitral valve anatomy amenable to repair given superior long-term outcomes demonstrated with successful mitral valve repair, preservation of left ventricular geometry, and more favorable left ventricular remodeling.2 The recurrence rate of MR after surgical mitral valve repair has been demonstrated to be higher in patients with isolated anterior leaflet pathology compared with those with isolated posterior leaflet or bileaflet pathology.3 Therefore, this patient is at higher risk for less favorable outcomes after surgical mitral valve repair.
References
Sorajja P, Mack M, Vemulapalli S, et al. Initial Experience With Commercial Transcatheter Mitral Valve Repair in the United States. J Am Coll Cardiol 2016;67:1129-40.
Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2016;63:e57-185.
Suri RM, Clavel MA, Schaff HV, et al. Effect of Recurrent Mitral Regurgitation Following Degenerative Mitral Valve Repair: Long-Term Analysis of Competing Outcomes. J Am Coll Cardiol 2016;67:488-98.