View other clinical content from the Bordeaux Group at:
Figures 1-4
A patient recipient of a Virtuoso DR implantable cardioverter-defibrillator (ICD) is hospitalized for syncope and electrical shock. This 73-year-old man, who presented with a stable dilated cardiomyopathy (with narrow QRS complexes and left ventricular ejection fraction assessed at 31% by echocardiogram) and documented episodes of VT, undergoes implantation of a Virtuoso dual chamber ICD. He is seen in the cardiac emergency department after receiving an electrical shock. Note that the patient did present with syncope before the shock, which was clearly noticed by his spouse who was scared by her husband's symptoms.
Which of the following statements describes the type of arrhythmia that the ICD identifies for therapy delivery?
Show Answer
The correct answer is: B. The device considers this arrhythmic episode as a VF, whereas it is a T-wave oversensing phenomenon, so that therapy is not adapted.
This tracing highlights the potential risks associated with inappropriate therapies delivered in the context of T-wave oversensing. Both shocks and antitachycardia pacing (ATP) may induce life-threatening ventricular arrhythmias since they can be delivered during the vulnerable period. Shocks are synchronized either on the R-wave either on the T-wave (50%/50%). As in this case, the first paced cycle of the ATP sequence can also correspond to the peak of the T-wave, explaining the induction of a real episode of VF. The diagnosis made by the device was initially wrong (false VF) but turned out to be finally correct after acceleration into a polymorphic ventricular arrhythmia.
Figures 1-4
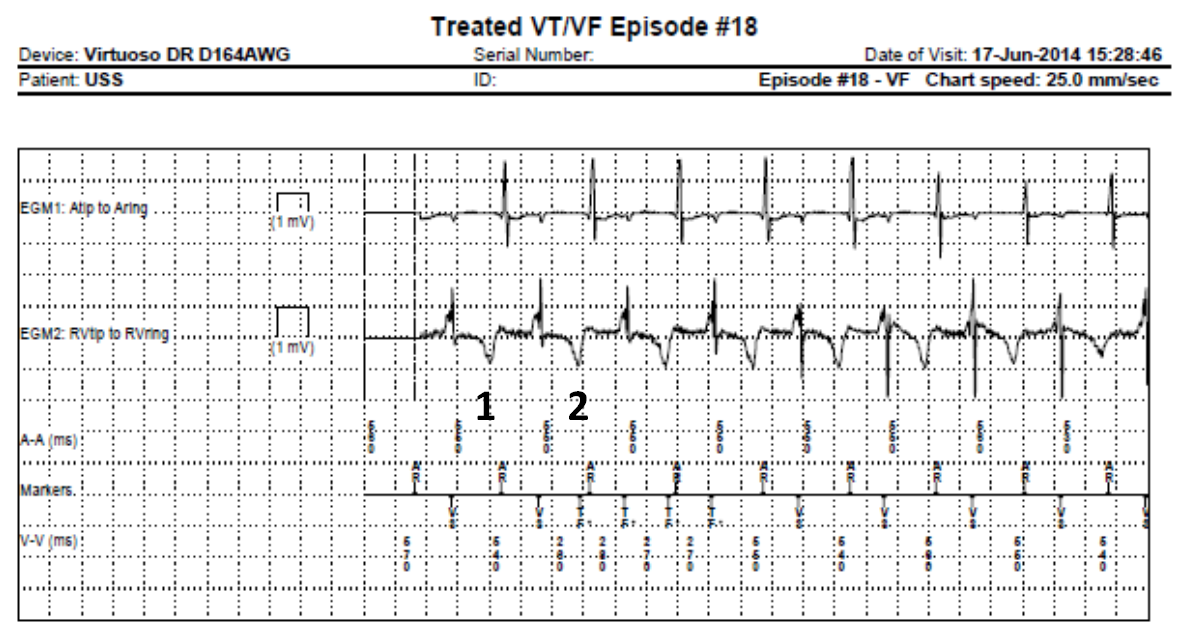
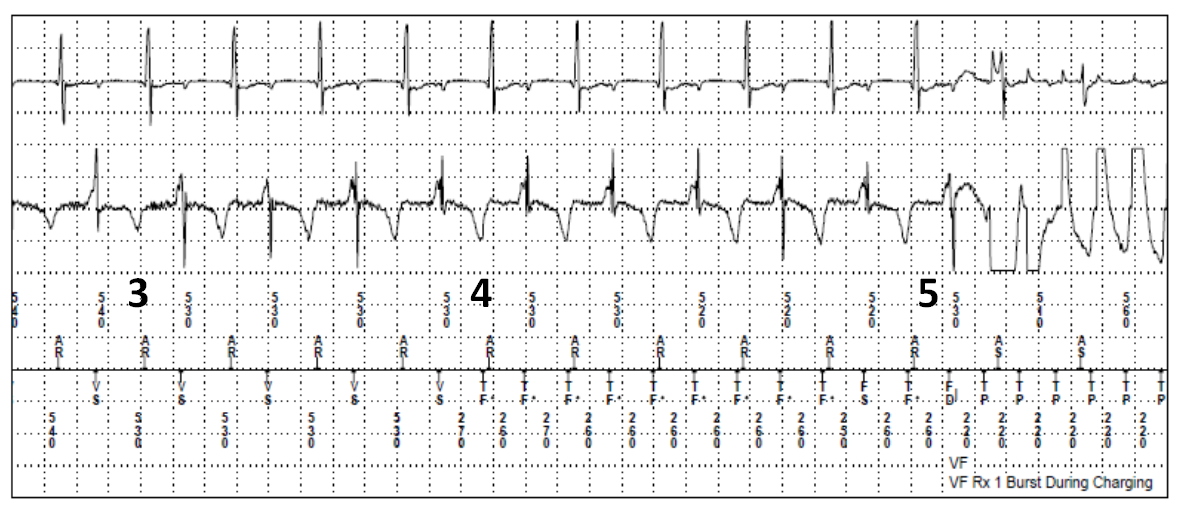
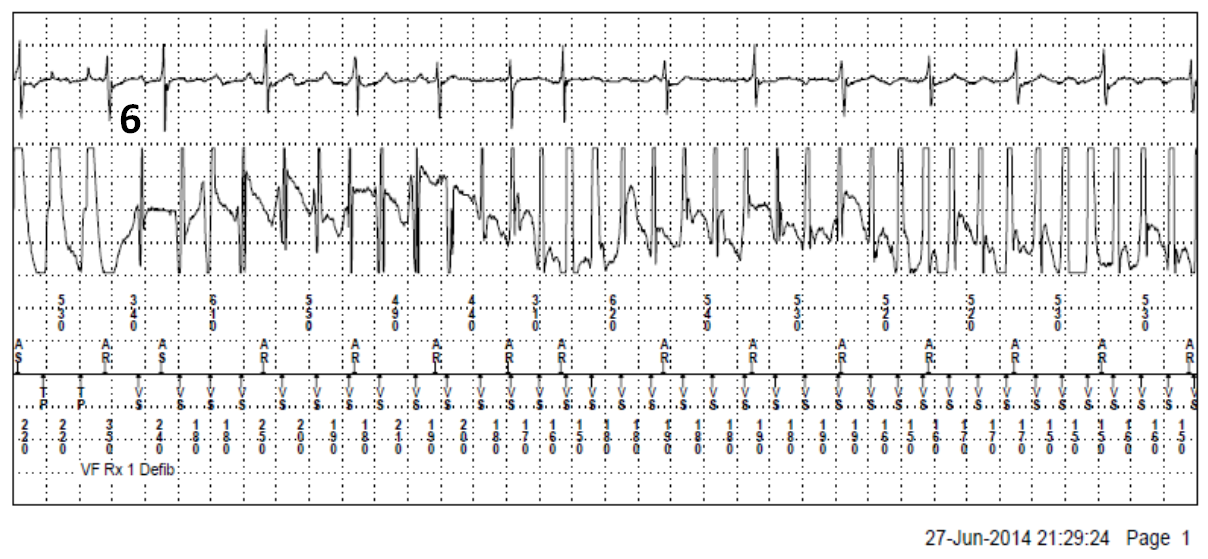
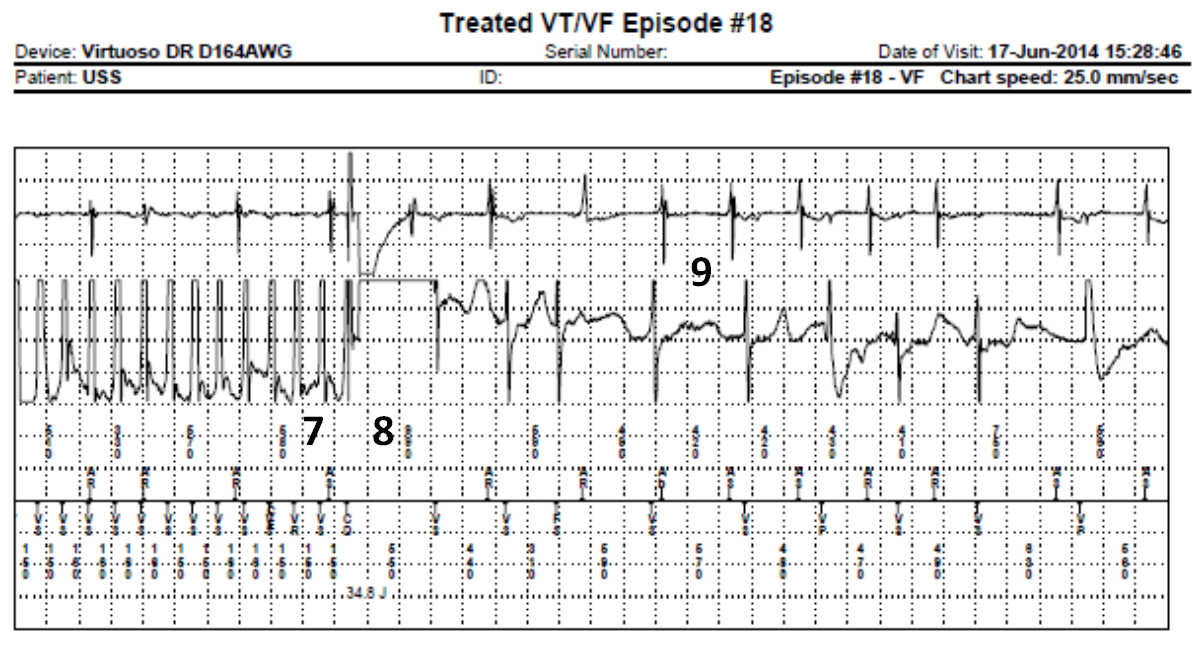
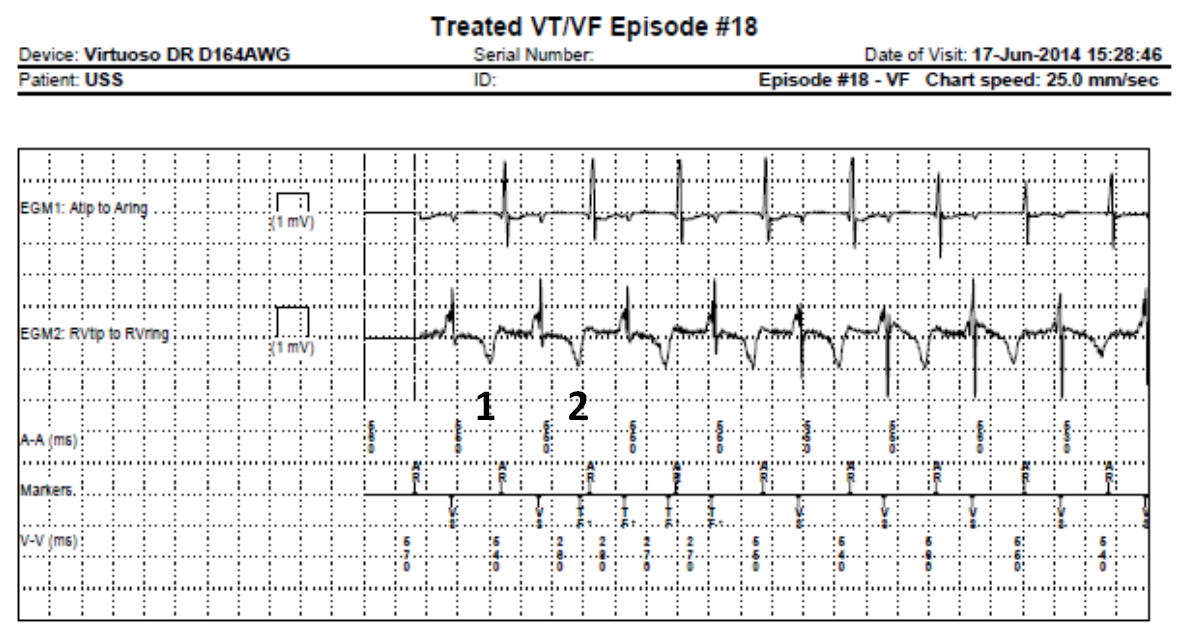
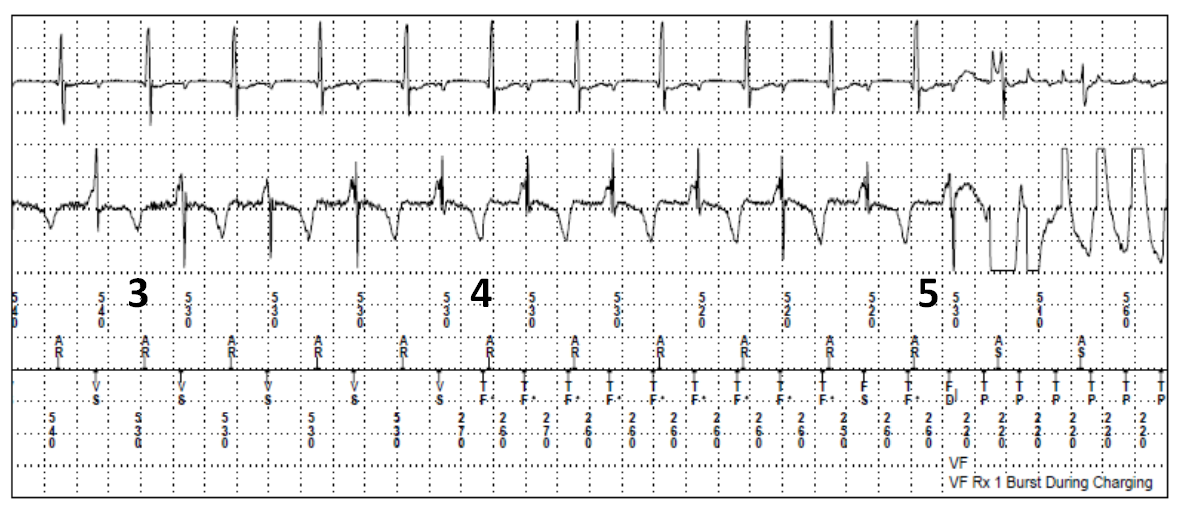
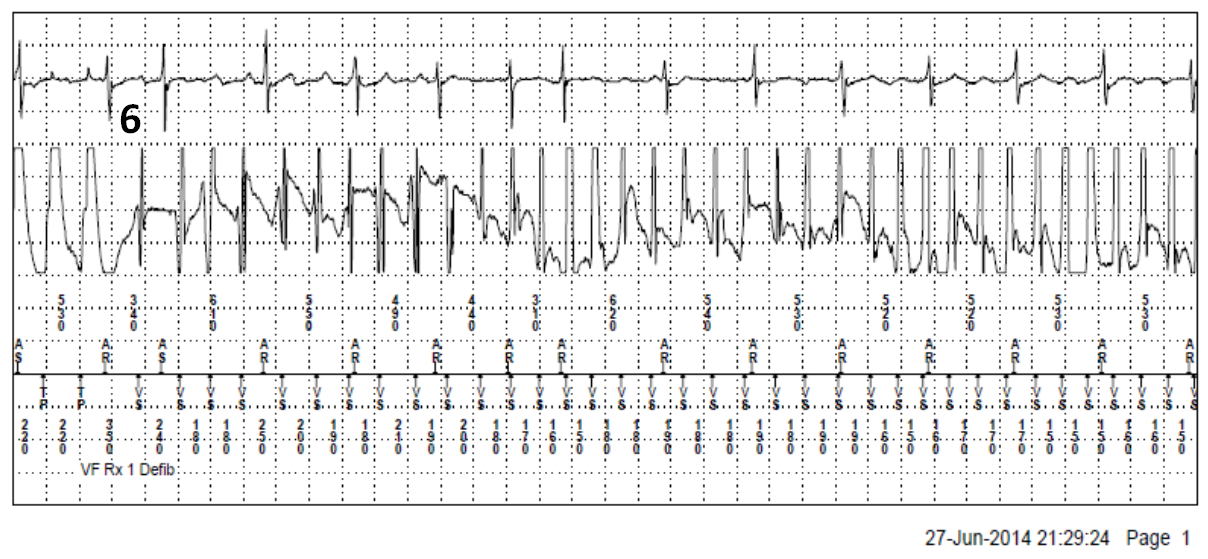
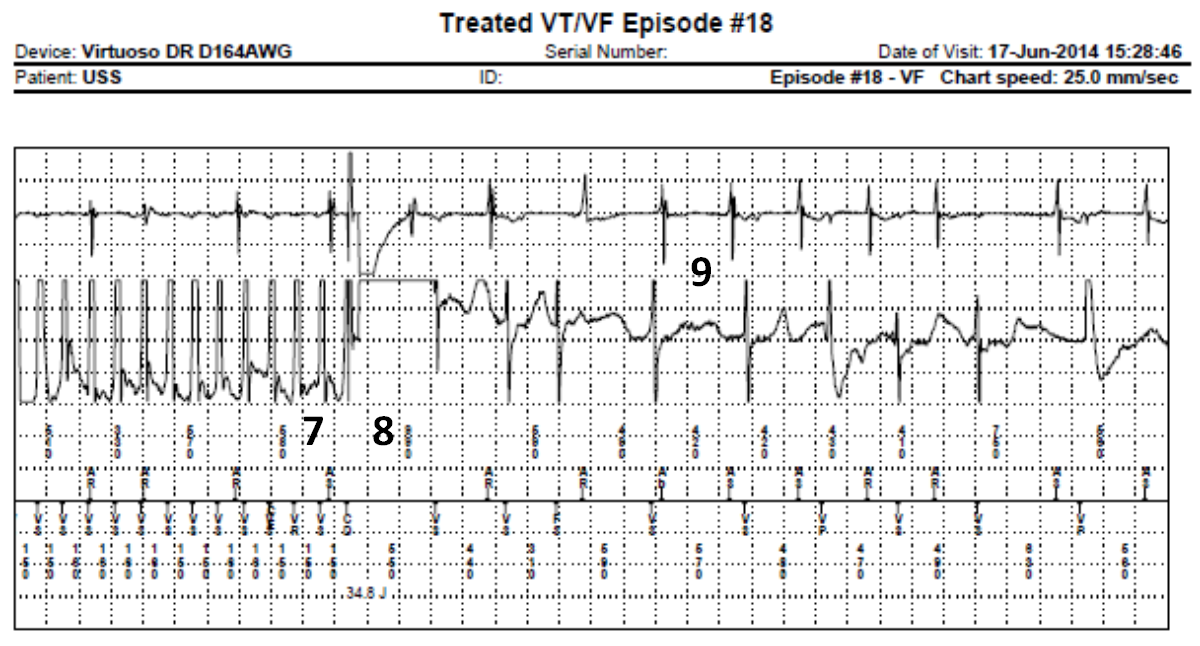
Episode Plot and Electrogram (EGM)
1: Sinus rhythm, with repetitive AR-VS cycles (extension of the PVARP to 400 ms, the device considering the ventricle cycle as a premature ventricular complex (PVC);
AR: Atrial sensing within the PVARP (post-ventricular atrial refractory period). VS: ventricular sensing out of any VT zone.
2: T-wave oversensing during two cycles;
3: Prolonged T-wave oversensing with nearly similar RT and TR intervals;
4: Diagnosis of VF; charge of the capacitors;
5: Burst during charging; the first paced cycle is delivered during the vulnerable period (between onset and peak of the T-wave);
6: Induction of a polymorphic, very fast ventricular arrhythmia;
7: At the end of charge, confirmation of the arrhythmia (the first cycle following the end of charge is labeled VR in relation to the short blanking duration related to the end of charge);
8: Shock delivered;
9: Return to sinus rhythm.
References
Groh CA, Sharma S, Pelchovitz DJ, et al. Use of an electrocardiographic screening tool to determine candidacy for a subcutaneous implantable cardioverter-defibrillator. Heart Rhythm 2014;11:1361-6.
Almehairi M, Somani R, Ellenbogen K, Baranchuk A. Inappropriate detection of ventricular fibrillation in the presence of T-wave oversensing algorithm. Pacing Clin Electrophysiol 2014 Apr 15. [Epub ahead of print]
Guédon-Moreau L, Kouakam C, Klug D, et al. Decreased delivery of inappropriate shocks achieved by remote monitoring of ICD: A substudy of the ECOST trial. J Cardiovasc Electrophysiol 2014;25:763-70.
Kooiman KM, Knops RE, Olde Nordkamp L, Wilde AA, de Groot JR. Inappropriate subcutaneous implantable cardioverter-defibrillator shocks due to T-wave oversensing can be prevented: Implications for management. Heart Rhythm 2014;11:426-34.