Valve-in-Valve TAVI With Postoperative High Gradient
A 77-year-old male presented with severe dyspnea. Medical history revealed quadruple aortocoronary bypass surgery and implantation of a 23 mm Medtronic Hancock porcine bioprosthesis (Medtronic, Minneapolis, MN) 6 years ago. Invasive angiography and echocardiograpy showed open quadruple bypass grafts, a severe reduced left ventricular function and stenosis grade III of the implanted porcine aortic valve with concomitant insufficiency grade II. Logistic Euroscore was 28.8%, STS Score 26.7%.
|
Two months later the patient was readmitted in cardiac decompensation. Re-angiography showed still open quadruple bypass grafts, but an invasive gradient of 50 mmHg over the Edwards Sapien valve.
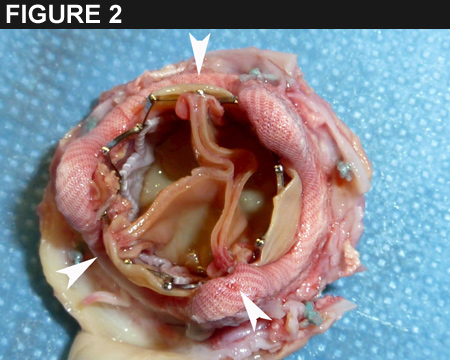
Echocardiography confirmed the severe stenosis of the aortic bioprosthesis with a maximum gradient of 66 mmHg, a mean of 43 mmHg and a valve opening area of 0.6 cm2 (Fig. 1).
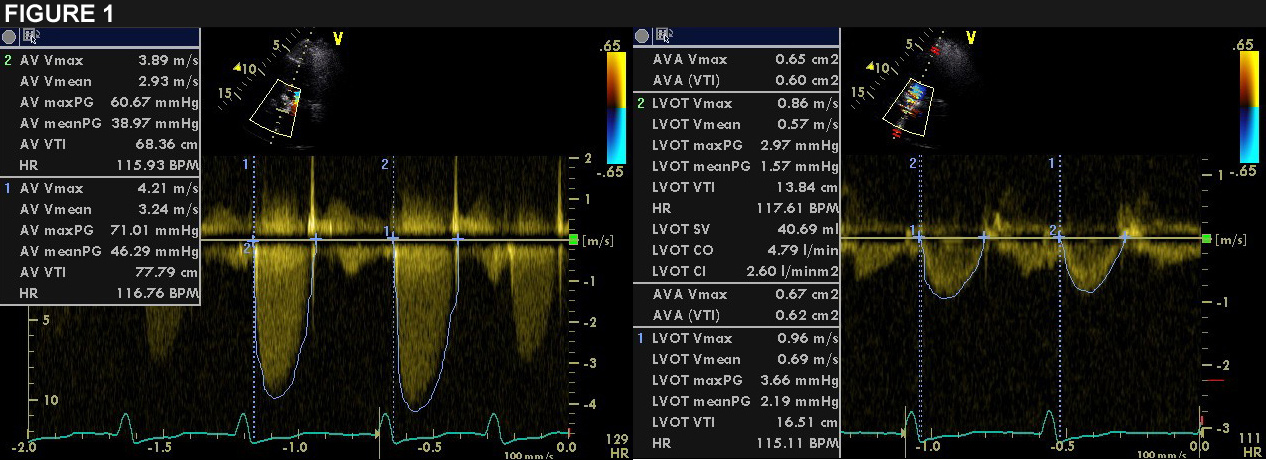
Both the Edwards Sapien valve-in-valve bioprothesis and the 2004 implanted Hancock bioprosthesis were surgical explanted and replaced with a 21 mm St. Jude Medical Trifecta (St. Jude Medical Inc, St. Paul, Minnesota) bioprosthesis.
What could be the reason for the high gradient of the valve-in-valve TAVI early after implantation?
Show Answer