A 57-year-old man with a prior medical history of hypertension, impaired fasting glucose, bicuspid aortic valve (undiagnosed until adulthood), and rheumatic heart disease with reduced left ventricular ejection fraction (LVEF) (22% at the time of presentation) was admitted to the hospital with shortness of breath. Fifteen years prior to his current presentation, the patient was diagnosed with bicuspid aortic valve and severe aortic insufficiency (AI) with reduced left ventricular (LV) systolic function (20%) and underwent a Ross procedure (aortic root replacement with pulmonary autograft). Postoperatively, he developed a large pseudoaneurysm (8 cm at its widest diameter) at the proximal aortic suture line, with communication into the LV outflow tract. He then underwent surgical aortic root replacement with a 23 mm CryoLife homograft (CryoLife, Inc.; Kennesaw, GA), approximately 2.5 months after his initial Ross procedure. At the time of discharge, his LVEF was 20% with mild aortic regurgitation (AR) and moderate pulmonary regurgitation (PR).
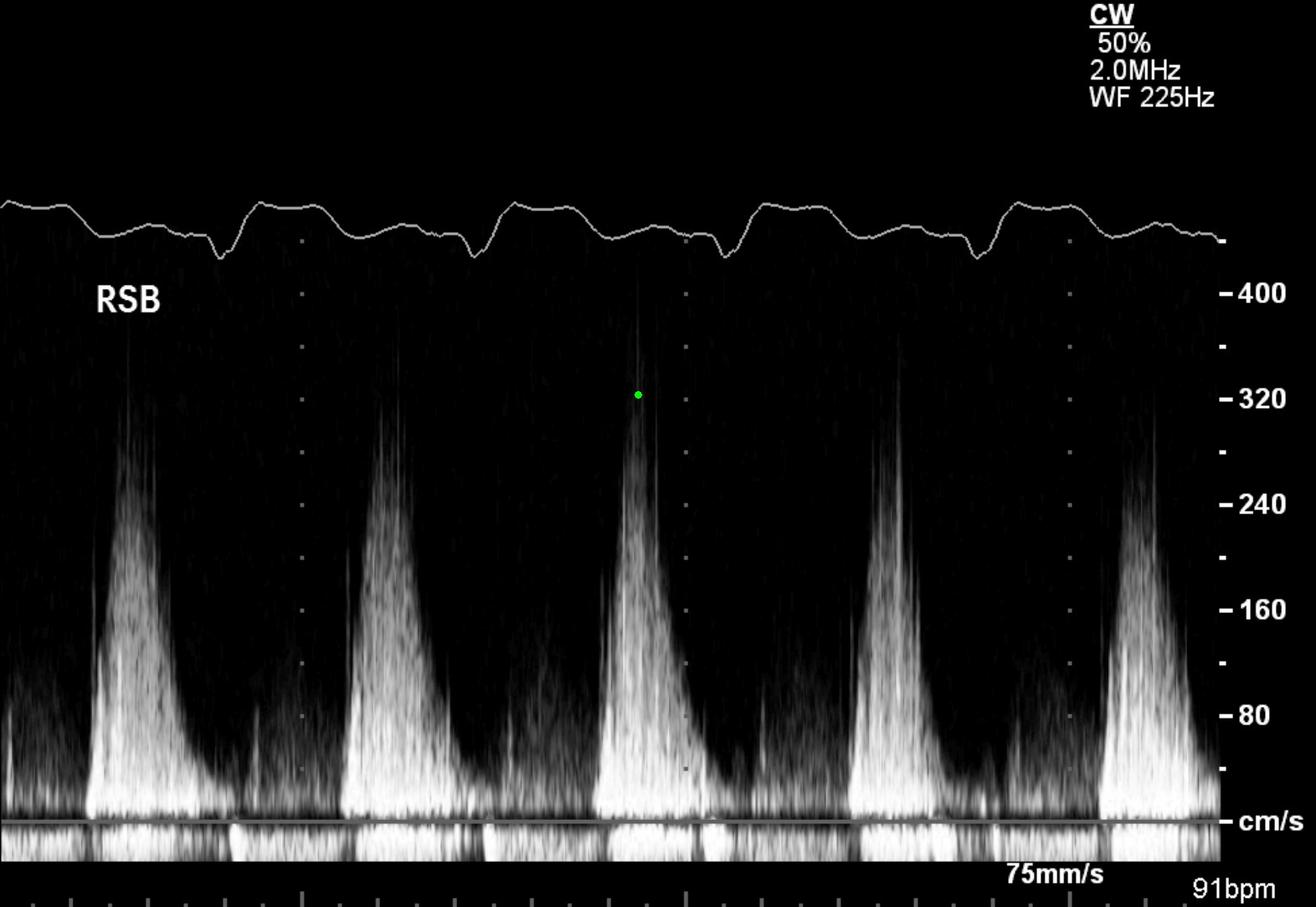
The patient did well for the next decade on medical therapy, with his LVEF improving to 55% 12 months after his homograft repair and root replacement. At approximately 4 months prior to the current presentation, the patient was hospitalized with volume overload; transthoracic echocardiogram showed aortic homograft stenosis (mean gradient = 21 mmHg) (Figure 1) with mild-to-moderate aortic regurgitation and LVEF of 26%. The patient was medically managed and discharged home. Over the ensuing months, despite attempts at medical therapy, the patient developed worsening dyspnea on exertion and reduced exercise intolerance. A repeat echocardiogram showed a mean gradient of 23 mmHg across the aortic valve with moderately severe AR (Videos 1-2). Given the patient's reduced LV systolic function (LVEF = 22% at this time) and prolonged QRS (150 ms), it was decided to pursue cardiac resynchronization therapy pacemaker implantation (the patient refused an implantable cardioverter-defibrillator) and subsequently he was also referred to the Heart Team for consideration of transcatheter aortic valve replacement (TAVR). After review by a cardiothoracic surgeon, the patient was felt to have low-flow, low-gradient hemodynamics and was at extreme surgical risk for aortic valve replacement given two prior sternotomy procedures with multiple interventions on his aortic root in the past.
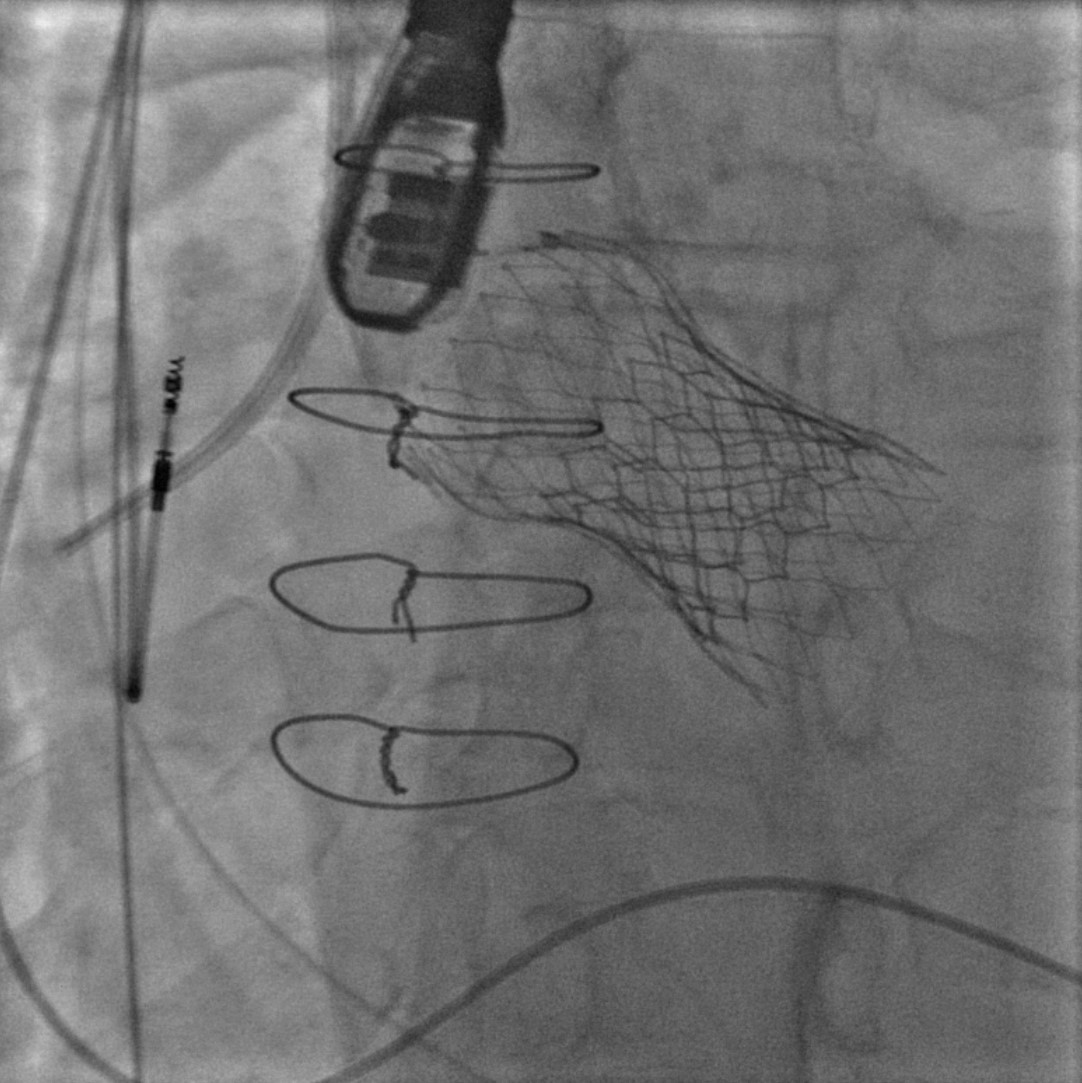
TAVR was thus pursued, with a self-expanding 29 mm Medtronic CoreValve Evolut R (Medtronic, Inc.; Minneapolis, MN) implanted via the transfemoral approach (Figure 2). Post-procedure, the patient developed severe paravalvular leak and intravalvular regurgitation after the valve was noted to migrate into the LV outflow tract (Videos 3-4). A balloon-expandable 29 mm Edwards SAPIEN 3 valve (Edwards Lifesciences, Inc.; Irvine, CA) was subsequently implanted via the transfemoral approach, with excellent result (Figure 3).
Figure 2
Aortogram showing successful TAVR of a self-expanding valve.
Video 3
Video 4
Figure 3
Aortogram showing successful TAVR of a balloon-expandable valve within a self-expanding TAVR valve.
Which of the following statements is true?
Show Answer
The correct answer is: D. Mortality rates of patients undergoing valve-in-homograft TAVR for aortic homograft failure are comparable to patients undergoing valve-in-valve TAVR for bioprosthetic aortic valve replacement failure.
Valve-in-homograft TAVR for patients with failed aortic homograft can be significantly more complex than for patients with native aortic valve stenosis. Multiple potential issues exist, including but not limited to precise and accurate sizing of the homograft annulus and navigating angulated and/or distorted anatomy of the surgically altered aortic root with respect to the rest of the native (and surgically naïve) aorta when delivering the transcatheter valve. Close attention must also be paid to whether the original surgical procedure included full root replacement along with homograft implantation or if a subcoronary implantation technique was employed.1 If full root replacement or an inclusion cylinder technique were initially used, this has been shown to maintain the sinotubular and commissural geometry of the aortic homograft and can lead to less AI.2 It is unclear if the surgical technique initially used to repair the failing valve has a later effect on TAVR and/or if a balloon-expandable versus a self-expanding bioprosthesis would be ideal in this scenario.1
Reoperation for homograft failure occurs in 10-25% of patients within 15 years of surgery, a rate that increases to an approximate 50% failure rate by 20 years post-surgery.3
Similar to the patient presented in the case above, valve-in-homograft procedures were initially primarily reported using the CoreValve bioprosthetic;4-6 however, both transapical and transfemoral approaches using the Sapien bioprosthetic have also been reported in literature with excellent results.1,7
Patients who have undergone aortic homograft very commonly develop failure over time, with insufficiency seen in up to 60% of patients, homograft stenosis developing in 17%, and endocarditis in 15.1%.8-11 Notably, mortality is similar to patients who have undergone other surgical aortic bioprosthetic valve implantation, at a published rate of approximately 3-8%.12,13 Aortic homograft failure is accelerated by patients with end-stage renal disease and on hemodialysis.14
Traditionally, when used in the treatment of aortic homograft failure, TAVR via surgical approach (i.e., thoracotomy and transapical, or sternotomy and direct aortic catheterization) was advocated as the treatment method of choice due to possible friability and concern for disruption of the homograft aortic root via the transfemoral approach.15 However, as discussed above, successful transfemoral TAVR in aortic homograft failure was later reported in literature.1
Knott-Craig CJ, Elkins RC, Stelzer PL, et al. Homograft replacement of the aortic valve and root as a functional unit. Ann Thorac Surg 1994;57:1501-5.
Sadowski J, Kapelak B, Bartus K, et al. Reoperation after fresh homograft replacement: 23 years' experience with 655 patients. Eur J Cardiothorac Surg 2003;23:996-1000.
Olsen LK, Engstrøm T, Søndergaard L. Transcatheter valve-in-valve implantation due to severe aortic regurgitation in a degenerated aortic homograft. J Invasive Cardiol 2009;21:E197-200.
López-Otero D, Teles R, Gómez-Hospital JA, et al. Transcatheter aortic valve implantation: safety and effectiveness of the treatment of degenerated aortic homograft. Rev Esp Cardiol (Engl Ed) 2012;65:350-5.
Pasic M, Buz S, Unbehaun A, Hetzer R. Transcatheter aortic valve implantation combined with conventional heart surgery: hybrid approach for complex cardiac pathologic features. J Thorac Cardiovasc Surg 2012;144:728-31.
Dainese L, Fusari M, Trabattoni P, Biglioli P. Redo in aortic homograft replacement: transcatheter aortic valve as a valid alternative to surgical replacement. J Thorac Cardiovasc Surg 2010;139:1656-7.
Barratt-Boyes BG, Roche AH, Subramanyan R, Pemberton JR, Whitlock RM. Long-term follow-up of patients with the antibiotic-sterilized aortic homograft valve inserted freehand in the aortic position. Circulation 1987;75:768-77.
O'Brien MF, Harrocks S, Stafford EG, et al. The homograft aortic valve: a 29-year, 99.3% follow-up of 1,022 valve replacements. J Heart Valve Dis 2001;10:334-44.
Yacoub M, Rasmi NR, Sundt TM, et al. Fourteen-year experience with homovital homografts for aortic valve replacement. J Thorac Cardiovasc Surg 1995;110:186-93.
Hasnat K, Birks EJ, Liddicoat J, et al. Patient outcome and valve performance following a second aortic valve homograft replacement. Circulation 1999;100:1142-7.
Joudinaud TM, Baron F, Raffoul R, et al. Redo aortic root surgery for failure of an aortic homograft is a major technical challenge. Eur J Cardiothorac Surg 2008;33:989-94.
Kumar P, Athanasiou T, Ali A, et al. Re-do aortic valve replacement: does a previous homograft influence the operative outcome? J Heart Valve Dis 2004;13:904-12.
London GM, Pannier B, Marchais SJ, Guerin AP. Calcification of the aortic valve in the dialyzed patient. J Am Soc Nephrol 2000;11:778-83.
Robicsek F, Thubrikar MJ. Conservative operation in the management of annular dilatation and ascending aortic aneurysm. Ann Thorac Surg 1994;57:1672-4.