View other clinical content from the Bordeaux Group at:
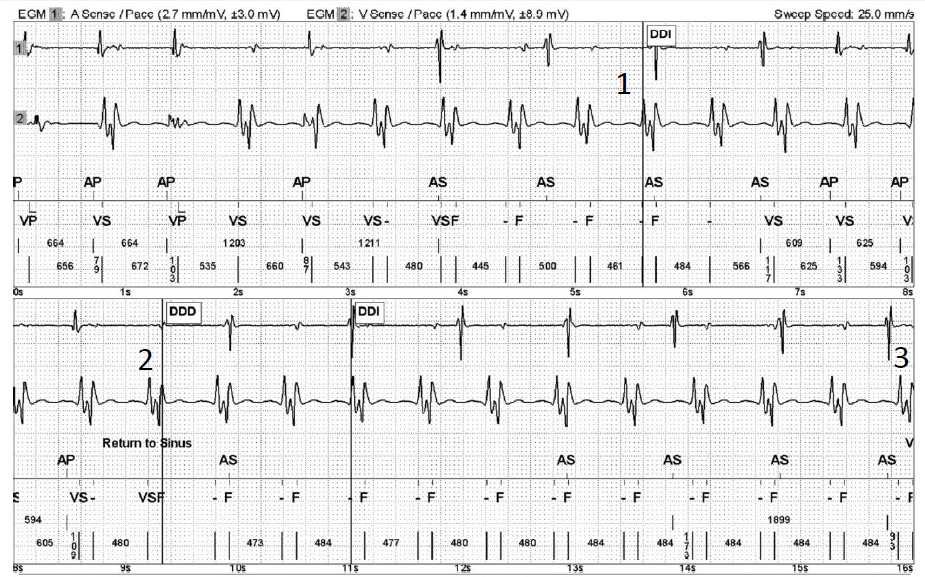
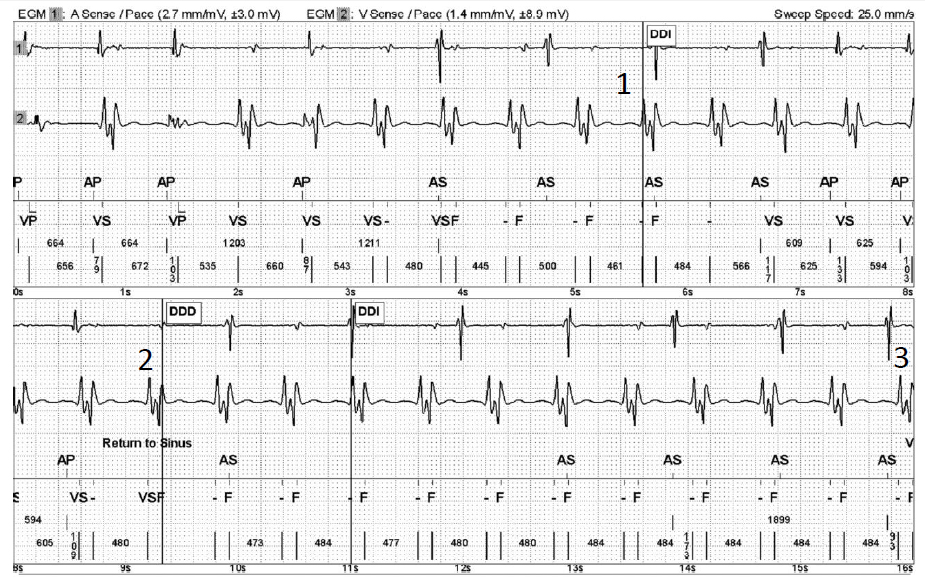
A 78-year-old man presents with a severely dilated cardiomyopathy and multiple episodes of slow ventricular tachycardia (VT), and undergoes implantation of an EpicTM dual-chamber implantable cardioverter-defibrillator (ICD). He was seen in consultation after receiving an electrical shock. Although the patient did not feel any dizziness or lipothymia before the shock delivery, he experienced shortness of breath. See Figures 1 and 2.
Figure 1
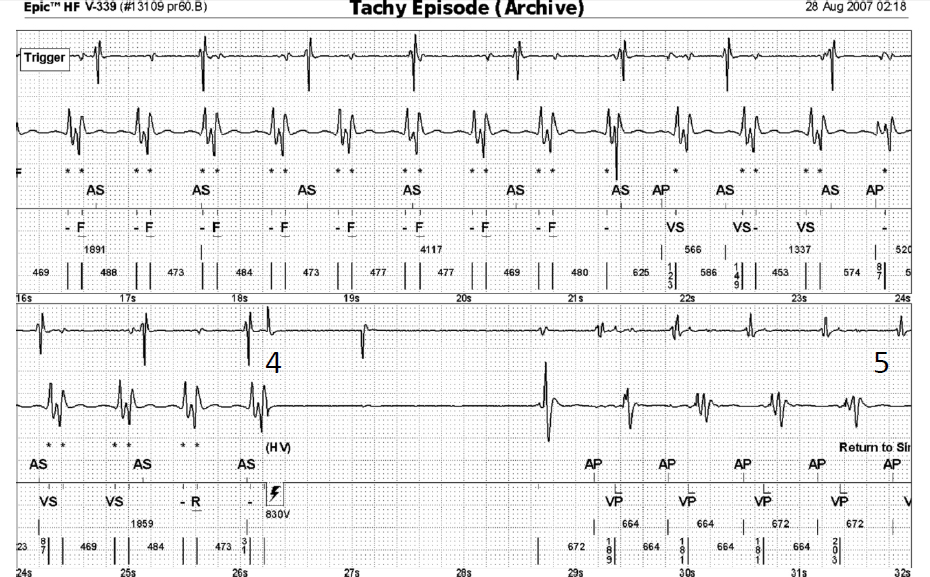
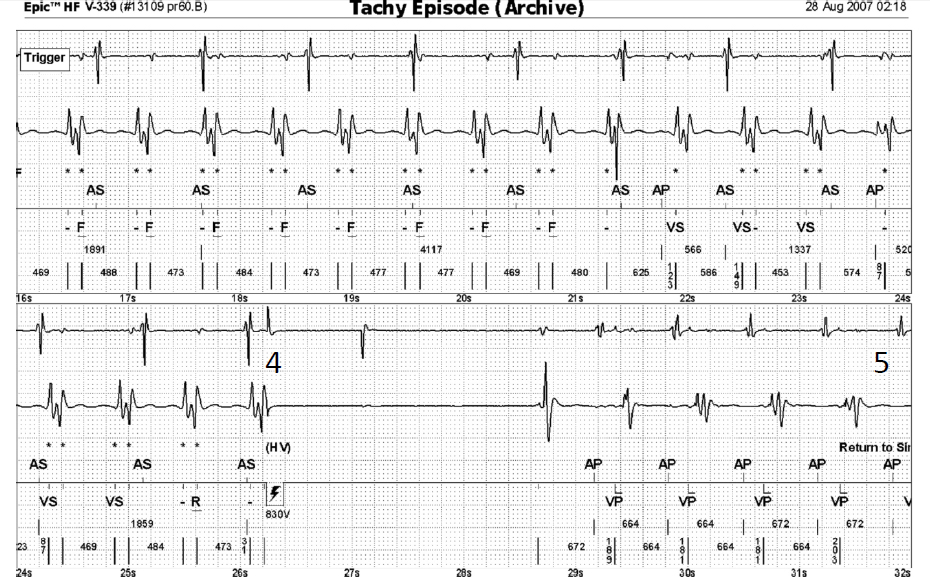
Figure 2
Which of the following statements describes the type of arrhythmia that the ICD identifies?
Show Answer
The correct answer is: C. Ventricular arrhythmia inappropriately identified by the ICD as VF due to the occurrence of ventricular event double counting by the ventricular ICD lead.
The VF episode detected via the combined counter (sensed events alternating between “-” and “F”) triggered a charge to 35 J in 6.2 sec. The first shock was diverted. Because of recurrence of oversensing, an episode of VF is redetected, prompting a second charge. Because the capacitors are partially charged, the charge time is shorter, and the shock is delivered.
The ICD analysis was not appropriate because an episode of VF was wrongly identified instead of a true episode of slow VT. Accordingly, the ICD has delivered a high-energy shock (VF zone programming) instead of providing ATP sequences (commonly used in a slow VT zone).
The reason is the occurrence of ventricular event double counting by the ventricular ICD lead.
Figure 1
Figure 2
Explanation of the Tracing
1: VT episode with AV dissociation. Very wide ventricular electrograms (EGMs) were sensed twice. The second ventricular EGM was sensed after the ventricular blanking period. The repetitive and regular alternation of long-short-long cycles suggests that a physiologic cardiac signal was oversensed.
2: Highly intermittent double counting and diagnosis of return of sinus rhythm.
3: Repetitive oversensing, detection of VF and charge of the capacitors (trigger and asterisks).
4: Electrical shock (HV, 830 V, 30 J).
5: Return to sinus rhythm without double counting after five ventricular paced (VP) events.
Comments
Double counting of the QRS complex can occur during sinus rhythm or during an episode of VT. It can be eliminated by lengthening the ventricular blanking period.1-4 At least theoretically, any change in the ventricular sensitivity should be followed by the induction of VF to confirm that the new programming is associated with the proper detection of VF. In this patient, the lengthening of ventricular blanking to 157 ms suppressed the double counting of multiple episodes of slow VT.
In case of intermittent oversensing of a physiological signal, the probability of receiving an inappropriate therapy depends on the different manufacturers and on the way the counters are functioning. In St. Jude Medical devices like in this tracing, half of the signals are unclassified, which is associated with a delay in the diagnosis of return to sinus rhythm. This is a good point in case of undersensing of a true VF but is associated with an increased risk of inappropriate therapy in case of oversensing.
References:
Persson R, Earley A, Garlitski AC, et al. Adverse events following implantable cardioverter defibrillator implantation: a systematic review. J Interv Card Electrophysiol 2014;40:191-205.
Gold MR, Weiss R, Theuns DA, et al. Use of a discrimination algorithm to reduce inappropriate shocks with a subcutaneous implantable cardioverter-defibrillator. Heart Rhythm 2014;11:1352-8.
Rajamani K, Goldberg AS, Wilkoff BL. Shock avoidance and the newer tachycardia therapy algorithms. Cardiol Clin 2014;32:191-200.
Rauwolf T, Guenther M, Hass N, et al. Ventricular oversensing in 518 patients with implanted cardiac defibrillators: incidence, complications, and solutions. Europace 2007;9:1041-7.