A 63-year-old woman with severe aortic stenosis and coronary artery disease underwent coronary artery bypass grafting and aortic valve replacement with a 19 mm bioprosthetic valve. Her postoperative course was uncomplicated, and an echocardiogram done 1 month postoperatively demonstrated a well-seated prosthetic valve in the aortic position with a peak gradient of 20 mmHg, a mean gradient of 10 mmHg, and no aortic regurgitation. Two years after surgery, she presented to an outpatient cardiology clinic complaining of dyspnea on exertion and two-pillow orthopnea for several weeks. She denied chest pain, palpitations, syncope, or lower extremity edema. Her past medical history was otherwise notable for type 2 diabetes mellitus, hypertension, peripheral artery disease, and mixed connective tissue disease. Her medications included amlodipine, hydrochlorothiazide, lisinopril, metformin, aspirin, atorvastatin, and plaquenil. Her vital signs were as follows: blood pressure of 156/62; pulse of 82 bpm; respiratory rate of 18; oxygen saturation of 98% on room air. On cardiovascular examination, the heart had a regular rhythm, S1 was normal, and S2 was split. A grade 3, mid-peaking, systolic, crescendo-decrescendo murmur was audible at the base and radiated to carotids. The jugular venous pressure was estimated at 9 cm H20 with no hepatojugular reflex. Mild crackles were appreciated in bases of the lungs. Her blood work revealed a hemoglobin of 10.9 g/dl, normal haptoglobin, and normal lactate dehydrogenase level. The patient was referred for a transthoracic echocardiogram (TTE) that revealed normal biventricular systolic function; presence of a bioprosthetic aortic valve with peak transaortic gradient of 55 mmHg and mean gradient of 32 mmHg, trace aortic regurgitation; estimated pulmonary artery systolic pressure of 57mmHg; thickening of anterior and posterior mitral leaflets with posterior mitral annular calcification; and mild-to-moderate mitral regurgitation. The maximum velocity across left ventricular outflow tract was 0.6m/sec; the maximum velocity across aortic valve was 3.6 m/sec; acceleration time of aortic valve was 115 milliseconds.
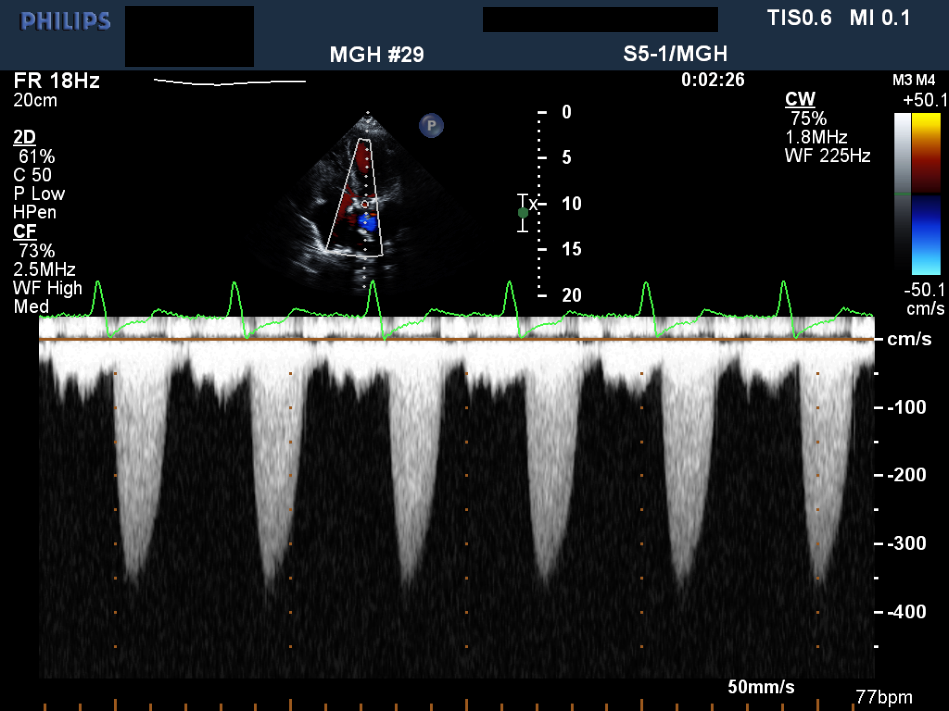
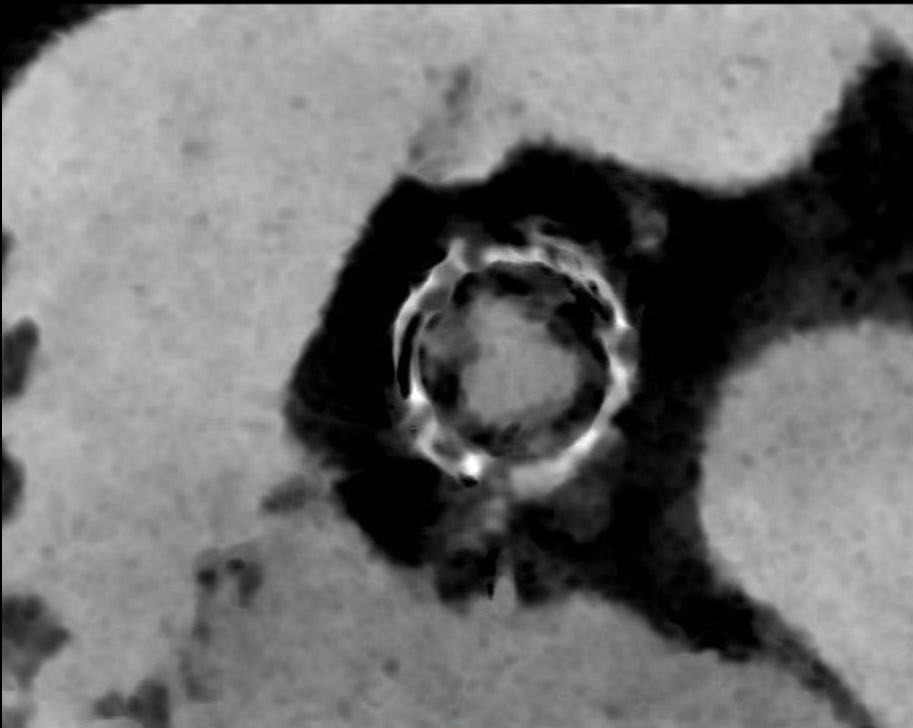
Shown below are the parasternal long axis (Video 1) and short axis views (Video 2) of the aortic valve on TTE, the transvalvular gradient Doppler profile on TTE (Figure 1), and radial multiplanar reconstruction (Figure 2) and axial minimum intensity projection (Figure 3) of aortic valve on cardiac computerized tomography (CT) scan.
Video 1
Video 2
Figure 1
Figure 2
Figure 3
What is the most likely etiology of increased transaortic valve gradients?
Show Answer
The correct answer is: B. Pannus formation
Given the small-sized valve, patient prosthesis mismatch is high in the differential diagnosis; however, one would expect immediate postoperative transvalvular gradients to be elevated. This patient had normal transaortic gradients in her postoperative echocardiogram. Thrombosis of prosthetic valves is more commonly seen in mechanical valves. Hemolysis is usually associated with mechanical valves and/or paravalvular regurgitation. Our patient had a bioprosthetic valve, normal haptoglobin level, and did not have any paravalvular regurgitation.
As outlined in the American Society of Echocardiography Guidelines on prosthetic valve evaluation, peak prosthetic aortic jet velocity > 3 m/sec requires further evaluation. The algorithm outlined in these guidelines recommend calculation of the Doppler velocity index (DVI) which is defined as the ratio of the proximal velocity in the left ventricular outflow tract to that of the flow velocity through the prosthetic valve. Significant prosthesis obstruction is considered when DVI is <0.25. The next step is qualitative assessment of the contour of velocity through the prosthesis. In normal valves, there is early peaking of the velocity with a short acceleration time, forming a triangular shape. Contrary to this, a more rounded contour is seen with a longer acceleration time in prosthetic valve obstruction. Acceleration time >100 milliseconds is useful in identifying stenotic valves. Our patient's echocardiogram showed a DVI of 0.17 (0.6 m/sec ÷ 3.6 cm/sec) and acceleration time of 115 m/sec, strongly suggesting significant prosthetic valve obstruction. Thrombosis and pannus formation are two common causes of prosthetic valve obstruction. Although the risk of bioprosthetic valve thrombosis was considered to be very low, recent studies suggest that it is not uncommon. Cardiac CT has been shown to be useful in differentiating thrombosis from pannus growth. In our case, radial multiplanar reconstruction (Figure 2) from an electrocardiography-gated cardiac CT demonstrated hypodense circumferential tissue growth at the inferior margin of the bioprosthetic aortic valve, consistent with pannus. Axial minimum intensity projection (Figure 3) with 5 mm thick reconstruction through the aortic valve prosthesis confirms circumferential pannus along the margins of the valve prosthesis.
Zoghbi WA, Chambers JB, Dumesnil JG, et al. Recommendations for evaluation of prosthetic valves with echocardiography and doppler ultrasound: a report From the American Society of Echocardiography's Guidelines and Standards Committee and the Task Force on Prosthetic Valves, developed in conjunction with the American College of Cardiology Cardiovascular Imaging Committee, Cardiac Imaging Committee of the American Heart Association, the European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography and the Canadian Society of Echocardiography, endorsed by the American College of Cardiology Foundation, American Heart Association, European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography, and Canadian Society of Echocardiography. J Am Soc Echocardiogr 2009;22:975-1014.
Egbe AC, Pislaru SV, Pellikka PA, et al. Bioprosthetic Valve Thrombosis Versus Structural Failure: Clinical and Echocardiographic Predictors. J Am Coll Cardiol 2015;66:2285-94.
Chung MS, Yang DH, Kim DH, Kang JW, Lim TH. Subvalvular pannus formation causing aortic stenosis in patient with a normal prosthetic aortic valve: computed tomography finding. Eur Heart J Cardiovasc Imaging 2015;16:458.