A 50-year-old Caucasian male with a history of obesity, poorly controlled hypertension, paroxysmal atrial fibrillation (PAF), diastolic dysfunction, and moderate obstructive sleep apnea (OSA) presents for follow-up in a multi-specialty sleep medicine clinic. His sleep study had an apnea hypopnea index (AHI) of 25 events per hour. He was prescribed continuous positive airway pressure (CPAP) therapy at 10 cm H2O pressure without additional oxygen supplementation. The patient has had the CPAP therapy for six months but has not followed up regularly. He reports having used the CPAP intermittently in the last 90 days. He states, "I just can't get used to the CPAP setup."
Figure 1
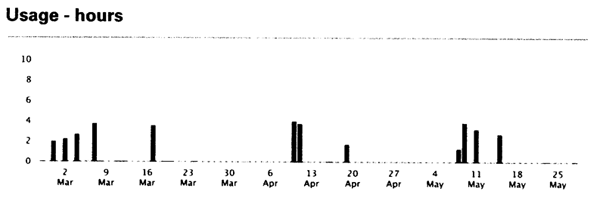
CPAP Usage
His CPAP usage is shown in Figure 1.
Over the last 90 days, CPAP adherence has been sporadic and less than four hours of usage on the nights CPAP was used. CPAP = continuous positive airway pressure.
Despite multiple attempts at adherence for appropriately prescribed CPAP therapy for the diagnosis of moderate OSA, this patient failed to comply with his therapy. He asks, "What other options do we have, and are they worth my time?"
Which of the following would you choose to help manage his OSA and potentially gain the optimal cardiovascular benefit?
Show Answer
The correct answer is: B. Try a mandibular advancement device (MAD) and/or enroll in weight loss program (exercise- and nutrition-based).
For patients who are prescribed positive pressure therapy to treat OSA, a significant portion is unable to tolerate CPAP. CPAP adherence is defined as a minimum of four hours of use per night and use of the machine for at least 70% of the nights in a given time period. Our patient's graph indicates that he is far from this threshold.
Studies have shown that patient experience in the first week of therapy is associated with CPAP adherence. Side effects associated with use of CPAP including oropharyngeal dryness, claustrophobia due to the mask, and noise of the machine can all lead to poor patient experience and contribute to non-adherence. Interventions (chinstrap, humidifier, placing CPAP machine on the carpet, mask adjustments, etc.) can help reduce these side effects and improve patient tolerance.1 Therefore these measures should be tried prior to moving to a MAD. The efficacy of MADs in treating mild-to-moderate OSA has been demonstrated in several published reports. There is not a large body of literature evaluating the effects of MADs on health outcomes. However, a recent observational study by Anandam et al. evaluated cardiovascular death in a non-concurrent cohort study of 570 patients with severe OSA.2 Patients who were non-adherent to CPAP were offered a MAD. After a median follow-up of 79 months, there was no difference in cardiovascular mortality when comparing patients with CPAP therapy versus MAD for OSA treatment. Patients with untreated OSA had a much higher cardiovascular mortality rate (2.1 per 100 person-years) compared to those who were treated for OSA (0.56 per 100 person-years in CPAP group and 0.61 per 100 person-years in MAD treated group). Thus answer option B should be offered to our patient who is unable to tolerate CPAP. Untreated OSA would expose our patient to increased cardiovascular morbidity and mortality with his history of uncontrolled hypertension and PAF. Therefore, answer option D should not be considered.
Benefits of weight loss through exercise and nutrition for OSA treatment have also been shown in various studies. In the systematic review and meta-analysis by Araghi et al., exercise- and diet-based interventions were effective at reducing AHI.3 In a recent study, Chirinos et al. evaluated the effect of blood pressure reduction in patients with sleep apnea using CPAP with or without concomitant weight loss therapy.4 With the combination of both CPAP adherence and weight loss, there was added improvement in blood pressure. Our patient would likely improve both his poorly controlled hypertension and improve his OSA with participation in a weight-loss program. Thus, the second half of answer option B should be offered regardless of CPAP compliance in obese patients.
Oxygen supplementation alone has not been shown to reduce AHI, although it has been shown to reduce hypoxemic episodes.5 Its effects on cardiovascular risk were recently tested in a study by Gottlieb et al. looking at CPAP versus oxygen in OSA.6 In this study, patients recruited from cardiology practices were shown to have a reduction in BP (despite being on least two antihypertensive medications on average) with the use of CPAP and not the use of supplemental oxygen. Therefore, answer option B is not likely to help with OSA or lead to cardiovascular benefits.
Drug therapies have been evaluated in select groups of patients. Fluticasone has been evaluated in patients with rhinitis and OSA. Donepezil has been evaluated in patients with dementia and OSA. In the Cochrane review by Mason et al., there was insufficient evidence to recommend the use of drug therapy in the treatment of OSA.7 Thus, answer option C is not the best answer.
References
Engleman HM, Wild MR. Improving CPAP use by patients with the sleep apnoea/hypopnoea syndrome (SAHS). Sleep Med Rev 2003;7:81-99.
Anandam A, Patil M, Akinnusi M, Jaoude P, El-Solh AA. Cardiovascular mortality in obstructive sleep apnoea treated with continuous positive airway pressure or oral appliance: an observational study. Respirology 2013;18:1184-90.
Araghi MH, Chen YF, Jagielski A, et al. Effectiveness of lifestyle interventions on obstructive sleep apnea (OSA): systematic review and meta-analysis. Sleep 2013;36:1553-62, 1562A-E.
Chirinos JA, Gurubhagavatula I, Teff K, et al. CPAP, weight loss, or both for obstructive sleep apnea. N Engl J Med 2014;370:2265-75.
Loredo JS, Ancoli-Israel S, Kim EJ, Lim WJ, Dimsdale JE. Effect of continuous positive airway pressure versus supplemental oxygen on sleep quality in obstructive sleep apnea: a placebo-CPAP-controlled study. Sleep 2006;29:564-71.
Gottlieb DJ, Punjabi NM, Mehra R, et al. CPAP versus oxygen in obstructive sleep apnea. N Engl J Med 2014;370:2276-85.
Mason M, Welsh EJ, Smith I. Drug therapy for obstructive sleep apnoea in adults. Cochrane Database Syst Rev 2013;5:CD003002.