A 27-year-old asymptomatic professional athlete presents for a cardiac evaluation after a preparticipation EKG stress test showed a 4 beat run of nonsustained ventricular tachycardia. He achieved 17 METs without symptoms. An echocardiogram demonstrated mildly enlarged right ventricle and mild left ventricular hypertrophy. Due to these abnormalities, a cardiac MRI was done and revealed partial absence of pericardium (Figure 1). A subsequent stress echocardiogram and Holter monitor was normal with only occasional ventricular premature beats. The athlete denied any episodes of chest pain, dyspnea, dizziness, syncope with rest or with heavy physical exertion. After review of his testing he was cleared for participation in professional sports without any restriction.
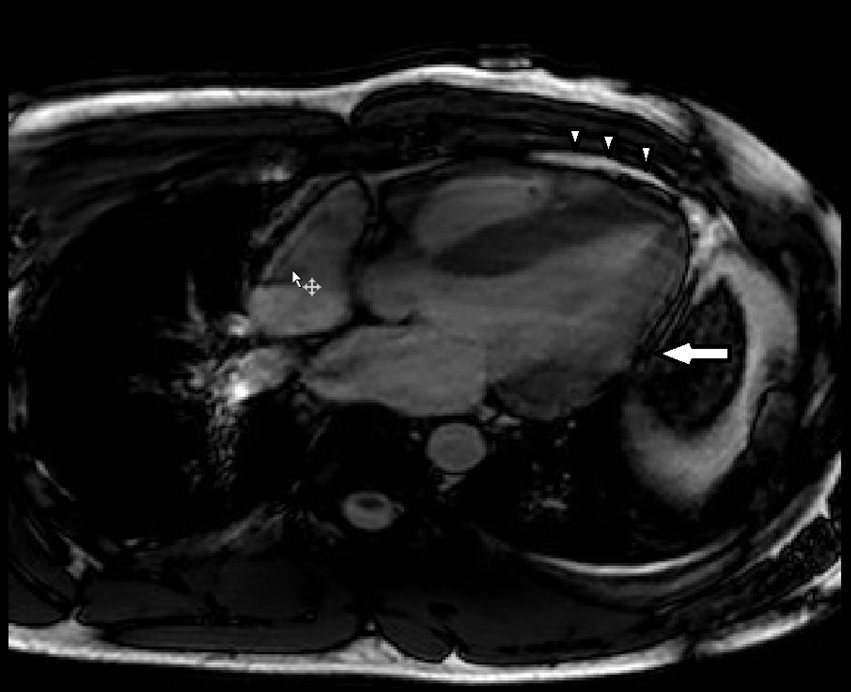
Figure 1
MRI SSFP cine image. Parietal and visceral pericardium is seen next to right ventricle and part of left ventricle (white arrow heads). There is absence of pericardium across the lateral wall of left ventricle (large white arrow).
All of the following are true statements regarding congenital absence of pericardium EXCEPT?
Show Answer
The correct answer is: D. Most patients require urgent surgical referral for complete pericardiectomy.
Statement D is incorrect as most patients with congenital absence of pericardium are asymptomatic and require no therapy.
Congenital absence of pericardium is a rare congenital anomaly. Failure of the pleuropericardial membranes to fuse and close the pleuropericardial cavity causes pericardial deficiencies, resulting in complete or, more commonly, partial absence of the pericardium. Most patients with congenital absence of pericardium are asymptomatic. Rarely patients may present with nonspecific symptoms of chest pain, dyspnea, or palpitations, although chest pain is the predominant symptom. Compression, herniation, or strangulation of cardiac chambers (most often the left atrial appendage), great vessels, or coronary arteries may occur in rare individuals. Indications for surgical repair include the presence of disabling symptoms or risk of occurrence of complications.
Statement A is correct. Partial absence of pericardium is more common than complete absence. Statement B and C are also correct.
Common imaging findings in congenital absence of pericardium are summarized in Table 1.
Table 1
Imaging Modality
Finding
Echo
Elongated tubular left ventricle “teardrop heart” from lack of tethering
Regional (apical) LV bulging during diastole – specific for partial absence (Video 1)
Unusual windows with posterior & left deviation of apex
CT/MRI
Absence of pericardial layer
Levorotation of the heart
Interposition of lung tissue in the anterior space between aorta and pulmonary artery or between the diaphragm and the base of the heart
Video 1
This echo video shows apical 4 chamber view from a 50-year-old male with history of partial congenital absence of pericardium. The apical window was very laterally displaced and the patient was supine at the time of this film acquisition. Note the regional bulging of the LV apex during diastole consistent with partial absence of pericardium.
References
Klein AL, Abbara S, Agler DA, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the Society for Cardiovascular Magnetic Resonance and Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. Sep 2013;26(9):965-1012 e1015.