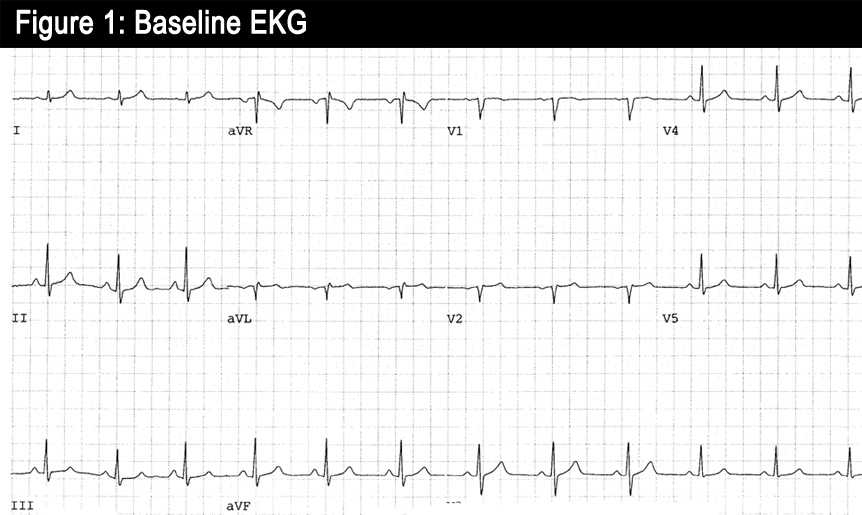
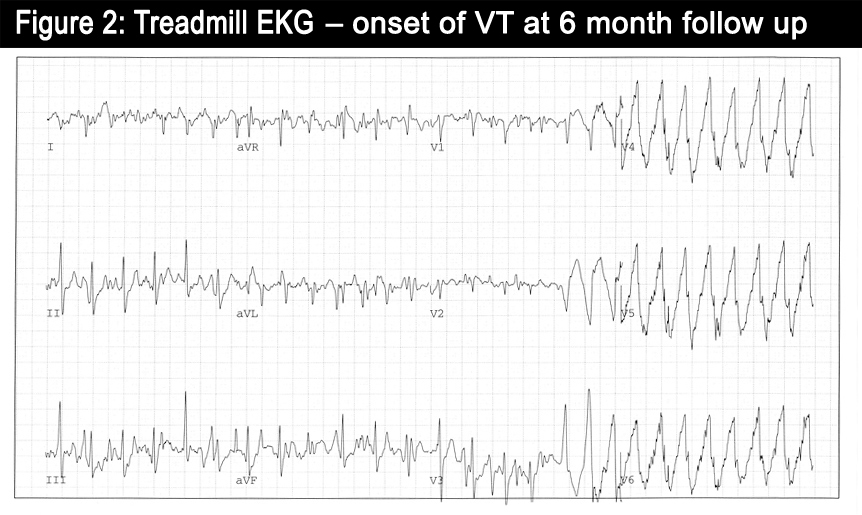
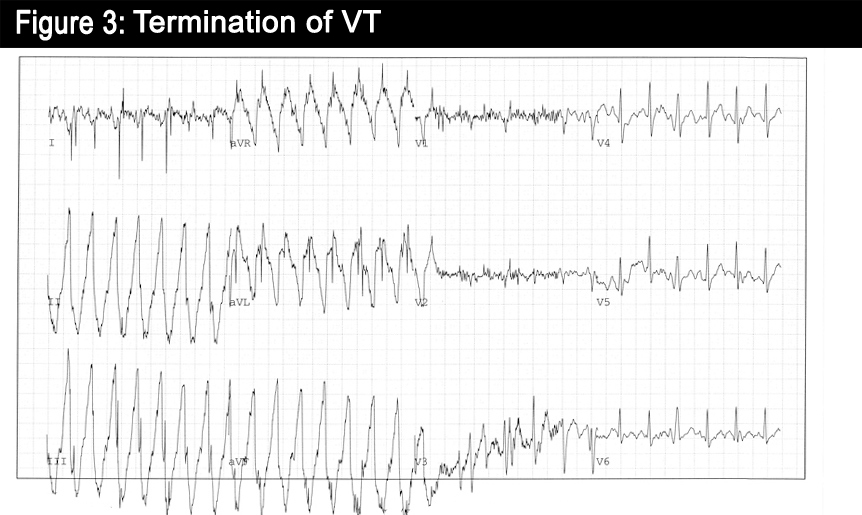
A 43-year-old previously healthy male, presents to cardiology clinic for episodes of dizziness and light-headedness while jogging. He was an avid runner for years, however, over the past few months, even with moderate jogging he gets light-headed and has to stop exercising. While he has not had a frank syncopal episode, he has become quite light-headed, with palpitations, and a "room spinning" sensation. His initial workup included an ECG with sinus bradycardia (Figure 1), and echocardiogram revealed a structurally normal heart with a normal ejection fraction. Baseline EKGExercise treadmill test revealed ventricular tachycardia 9 minutes into the Bruce Protocol at 9 mets. An MRI showed a structurally normal heart without evidence of scar tissue, hypertrophy, or other abnormalities. A coronary CT angiogram showed normal coronary arteries. He was placed on a beta-blocker, and was advised to avoid excessive caffeine and strenuous exercise. At the 6-month follow-up visit, he reported having symptoms sporadically despite his lifestyle modifications and titrating the beta-blocker to a resting heart rate in the 50s. His physician referred him again for an exercise treadmill test. After exercising for 13 minutes he became dizzy and had a run of non-sustained ventricular tachycardia (Figures 2 and 3). The treadmill test was aborted and his ventricular tachycardia spontaneously self terminated.
Based on the above information, the next most appropriate step would be:
Show Answer
The correct answer is: C. Catheter ablation of the ventricular tachycardia (VT).
This patient has idiopathic VT syndrome likely repetitive monomorphic VT (RMVT). These often arise from right ventricular outflow tract (RVOT), left ventricular outflow tract (LVOT), or fascicles. Many can be precipitated by exercise, and are often catecholamine or adenosine sensitive. These typically occur in structurally normal hearts and have a more benign prognosis.(1-3)
RMVT commonly presents as palpitations and lightheadedness during or immediately after exercise or emotional stress; however, a significant proportion of patients are asymptomatic.(4) Most RMVT episodes have a characteristic ECG appearance with left bundle-branch block appearance and an inferior axis. Catheter ablation is a Class I recommendation in patients with structurally normal hearts with symptomatic, drug-refractory VT arising from the RV or LV.(5) Also, ablation may be indicated in those who, like the described patient, are young and do not desire long-term drug therapy, or are drug intolerant, or who do not wish to curtail their exercise.(5)
The overwhelming concern in a patient with idiopathic ventricular tachycardia is sudden cardiac death (SCD). SCD occurs in patients without coronary artery disease or cardiomyopathy 5-10% of the time, and several forms of VT, including polymorphic catecholaminergic VT (CPVT), as well as sudden death due to other electrical disease such as LQT or Brugada syndromes, can precipitate SCD without overt structural changes in the heart.(5, 6) Fortunately, in otherwise healthy people without structural heart disease, VT arising from the RVOT, identifiable by its classic LBBB/inferiorly-directed axis with a normal ECG during sinus rhythm, is the most common form of VT and is associated with a good prognosis.(4, 5, 7) Drug therapy of symptomatic RMVT is a Class IIa recommendation that can involve beta-blockers, calcium channel blockers, or Type IC antiarrythmic drugs.(4, 5, 8, 9) In patients who remain symptomatic despite drug therapy, or those who do not wish to take medications, catheter ablation of the arrhythmia focus in the RVOT should be considered. Acute success rates for RMVT is quite good and for RVOT ablation success rate is typically greater than 90%.(10, 11) In this case, this patient was referred for ablation as he has failed maximal beta blocker therapy, was young and did not wish long term Class I drug.
References
Callans DJ, Menz V, Schwartzman D, et al. Repetitive monomorphic tachycardia from the left ventricular outflow tract: electrocardiographic patterns consistent with a left ventricular site of origin. J Am Coll Cardiol 1997; 29:1023.
Coumel P, LeClerq JP, Slama R. monomorphic idiopathic ventricular tachycardia. In: Cardiac Electrophysiology and Arrhythmias. Zipes DP, Jalife J (Eds). Grune and Stratton, Orlando 1985. p.455.
Coggins DL, Lee RJ, Sweeney J, et al. Radiofrequency catheter ablation as a cure for idiopathic tachycardia of both left and right ventricular origin. J Am Coll Cardiol 1994; 23:1333.
Buxton AE, Waxman HL, Marchlinski FE, et al. Right ventricular tachycardiaclinical and electrophysiologic characteristics. Circulation 1983; 68:917-927
Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. J Am Coll Cardiol 2006; 48:247-346.
Priori SG, Napolitano C, Memmi M, et al. Clinical and molecular characterization of patients with catecholaminergic polymorphic ventricular tachycardia. Circulation 2002; 106:69-74
Niroomand F, Carbucicchio C, Tondo C, et al. Electrophysiological characteristics and outcome in patients with idiopathic right ventricular arrhythmia compared with arrhythmogenic right ventricular dysplasia. Heart 2002; 87:41-47.
Krittayaphong R, Bhuripanyo K, Punlee K, et al. Effect of atenolol on symptomatic ventricular arrhythmia without structural heart disease. A randomized placebo-controlled study. Am Heart J 2002; 144:e10.
Gill JS, Blaszyk K, Ward DE, et al. Verapamil for the suppression of idiopathic ventricular tachycardia of left bundle branch block-like morphology. Am Heart J 1993; 126:1126-1133.
Morady F, Kadish AH, DiCarlo L, et al. Long-term results of catheter ablation of idiopathic right ventricular tachycardia. Circulation 1990; 82:2093-2099.
Coggins DL, Lee RJ, Sweeney J, et al. Radiofrequency catheter ablation as a cure for idiopathic tachycardia of both left and right ventricular origin. J Am Coll Cardiol 1994; 23:1333-1341.