2014 Hot Topic: Rollout of the MitraClip
The first percutaneous mitral repair procedures using the MitraClip device were done in 2003. MitraClip received FDA approval in October 2013 for use in patients with degenerative MR, who are at prohibitive risk for conventional mitral valve surgery. The device is the first in the class of percutaneous approaches for mitral regurgitation (MR). Several trials led to the approval, and the commercial rollout is underway.
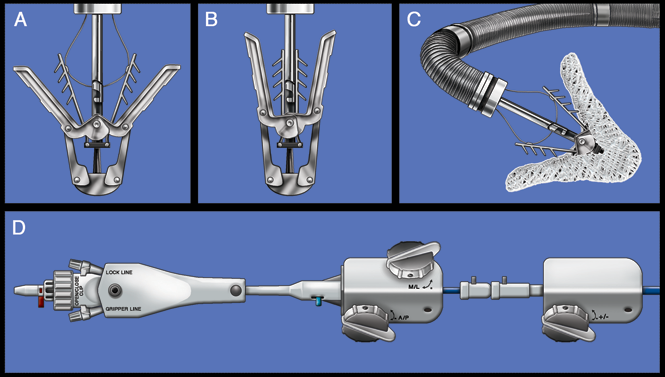 |
| Figure 1: The MitraClip System: (A) The partially open MitraClip device is shown without it's fabric covering. A fine wire runs through the barbed "grippers", which is used to raise the grippers. (B) The device in closed configuration. (C) The MitraClip is attached to the clip delivery system (CDS), which protrudes from the steerable guide catheter. (D) Control knobs allow deflection of the guide and CDS to steer the system through the left atruim and position the MitraClip above the mitral orifice. From: Feldman T, Young A: Percutaneous Approaches to Valve Repair for Mitral Regurgitation. J Am Coll Cardiol (2014). [Epub Ahead of Print]. doi: 10.1016/j.jacc.2014.01.039. |
The initial randomized comparison of percutaneous mitral repair with conventional mitral valve surgery (EVEREST II Trial- Endovascular Valve Edge-to-Edge Repair Study) set the stage for further development. This trial was performed in 279 candidates for conventional mitral valve repair surgery, predominantly with degenerative MR. Subjects were randomized to the device compared to surgical repair or replacement. The trial demonstrated that percutaneous repair is less effective at reducing MR than surgery, is safer than surgery, and ultimately results in similar improvements in quality of life and clinical status. Left ventricular dimensions and volumes were reduced with MitraClip. Patients with acute procedure success have durable results lasting as long as five years.
During the course of EVEREST II enrollment it was recognized that there is a population of older, frail patients with multiple comorbid conditions who are not responsive to medical management and are not candidates for any form of surgical therapy. These patients all had exclusions from the randomized trial. Many were noted to otherwise be suitable candidates for MitraClip. This led to the EVEREST High Risk Registry (HRR). Three hundred and fifty-one patients were studied in the non-randomized HRR. More than two-thirds of this group has functional rather than degenerative MR. The experience in the high-risk group has demonstrated that the procedure can be performed with a high level of safety and procedural success. These patients have reductions in left ventricular chamber volumes and dimensions, and significant clinical improvement. Importantly, the rate of heart failure hospitalizations per year is reduced by about half in this group of patients.
MitraClip received CE Mark approval in 2008 and has been utilized in over 12,000 patients worldwide. The international experience with MitraClip therapy parallels the high-risk registry experience from the US cohort. The technique and performance of the procedure has benefitted from the larger experience. The immediate procedure success rates now approach 100%. Thirty day mortality is low, especially considering the high-risk nature of these patients. Despite the older age and comorbidities of the treated patients more than 85% are discharged to home, without need for rehab. The majority of patients experience symptomatic improvement.
None of this prior high-risk patient experience prospectively separated functional and degenerative etiologies of MR, or included a randomized comparison with medical therapy. The COAPT (Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy for Extremely High-Surgical-Risk Patients) trial is examining the safety and effectiveness of the MitraClip device in high surgical risk patients with functional MR and heart failure, who are being randomized to either percutaneous mitral repair or to a control group with standard medical therapy alone. All pateints are evaluated for CRT before randomization. The primary endpoint is the rate of heart failure hospitalizations in the first year after therapy. A similar trial in Europe, RESHAPE-HF (A Randomized Study of the MitraClip Device of Heart Failure Patients with Clinically Significant Functional Mitral Regurgitation) is taking place.
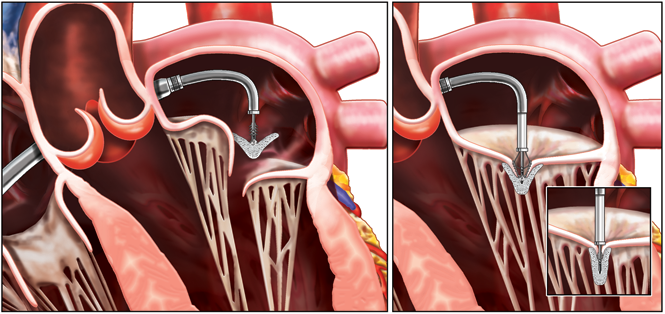 |
| Figure 2: To introduce the Clip, the Clip Delivery System (CDS) is advanced through the Guide into the left atrium (Left). Under echocardiographic and fluoroscopic guidance, the Clip is aligned perpendicular to the valve plane, with the Clip Arms perpendicular to the line of coaptation. It is then advanced into the left and then slowly retracted to grasp the leaflets (Right). The Clip is closed (Right, inset), and if reduction of mitral regurgitation is satisfactory, it is released. From: Feldman T, Young A: Percutaneous Approaches to Valve Repair for Mitral Regurgitation. J Am Coll Cardiol 2014. [Epub Ahead of Print]. doi: 10.1016/j.jacc.2014.01.039. |
The specific indication for use (www.abbottvascular.com/ifu) is, "The MitraClip Clip Delivery System is indicated for the percutaneous reduction of significant symptomatic mitral regurgitation (MR ≥ 3+) due to primary abnormality of the mitral apparatus [degenerative MR] in patients who have been determined to be at prohibitive risk for mitral valve surgery by a heart team, which includes a cardiac surgeon experienced in mitral valve surgery and a cardiologist experienced in mitral valve disease, and in whom existing comorbidities would not preclude the expected benefit from reduction of the mitral regurgitation."
The instructions for use (IFU) further defines prohibitive risk. Prohibitive risk is determined by the clinical judgment of a heart team, including a cardiac surgeon experienced in mitral valve surgery and a cardiologist experienced in mitral valve disease, due to the presence of one or more of the following documented surgical risk factors:
- 30-day STS predicted operative mortality risk score of ≥8% for patients deemed likely to undergo mitral valve replacement or ≥6% for patients deemed likely to undergo mitral valve repair
- Porcelain aorta or extensively calcified ascending aorta.
- Frailty (assessed by in-person cardiac surgeon consultation)
- Hostile chest
- Severe liver disease / cirrhosis (MELD Score >12)
- Severe pulmonary hypertension (systolic pulmonary artery pressure >2/3 systemic pressure)
- Unusual extenuating circumstance, such as right ventricular dysfunction with severe tricuspid regurgitation, chemotherapy for malignancy, major bleeding diathesis, immobility, AIDS, severe dementia, high risk of aspiration, internal mammary artery (IMA) at high risk of injury, etc.
- Evaluable data regarding safety or effectiveness is not available for prohibitive risk DMR patients with an LVEF < 20% or an LVESD > 60mm.
- MitraClip should be used only when criteria for clip suitability for DMR have been met.
- The major clinical benefits of MitraClip are reduction of MR to ≤2+ resulting in reduced hospitalizations, improved quality of life, reverse LV remodeling and symptomatic relief in patients who have no other therapeutic option. No mortality benefit following MitraClip therapy has been demonstrated.
- The heart team should include a cardiac surgeon experienced in mitral valve surgery and a cardiologist experienced in mitral valve disease and may also include appropriate physicians to assess the adequacy of heart failure treatment and valvular anatomy.
- The heart team may determine an in-person surgical consult is needed to complete the assessment of prohibitive risk. The experienced mitral valve surgeon and heart team should take into account the outcome of this surgical consult when making the final determination of patient risk status.
- For reasonable assurance of device effectiveness, pre-procedural evaluation of the mitral valve and underlying pathologic anatomy and procedural echocardiographic assessment are essential.
A post approval study of at least 2000 patients is required by FDA, and will be housed in the National Transcatheter Aortic Valve Replacement (TVT) registry housed jointly by the American College of Cardiology and Society for Thoracic Surgeons.
Recommendations for credentialing operators and institutions have not been published at the time of this writing, but will have many similarities to the criteria adopted for TAVR. For interventional operators, evidence of completion of device training as well as experience of 50 structural procedures per year (excluding ASD and PFO) and 15 transseptal procedures per year are recommended. Surgical programs will have a recommended mitral valve procedure minimum annual volume.
Since commercialization of the MitraClip, as of Martch 1, 2014, 155 procedures were performed at 31 sites.
References
- Feldman T, Wasserman HS, Herrmann HC, Gray W, Block PC, Whiltlow PL, St. Goar F, Rodriguez L, Silvestry F, Schwartyz A, Sanborn TA, Condado JA, Foster E: Percutaneous Mitral Valve Repair Using The Edge-to-Edge Technique: 6 Month Resultsof the EVEREST Phase I Clinical Trial. J Am Coll Cardiol 46:2134-40, 2005.
- Feldman T, Mauri L, Kar S, Fail P, Rinaldi M, Smalling R, Hermiller J, Gray W, Foster E Glower D on behalf of the EVEREST II Investigators. Final Results of the EVEREST II Randomized Controlled Trial of Percutaenous and Surgical Reduction of Mitral Regurgitation. Presented at ACC 2014.
- Feldman T, Alfieri O, St. Goar F: Percutaneous Leaflet Repair for Mitral Regurgitation Using the Evalve Edge-to-Edge Clip Technique, in Transcatheter Valve Repair, Eds Hijazi Z, Bonhoeffoer P, Feldman T, Ruiz C, Martin Dunitz & Parthenon Publishing/Taylor & Francis Medical Books, London, p 275-284, 2006.
- Feldman T, Kar S, Rinaldi M, Fail P, Hermiller J, Smalling R, Whitlow PL, Gray W, Low R, Herrmann HC, Lim S, Foster E, Glower D: Percutaneous Mitral Repair with the MitraClip System: Safety and Midterm Durability in the Initial EVEREST Cohort, J Am Coll Cardiol 54:686-694, 2009.
- Feldman T, Foster E, Glower D, Kar S, Rinaldi MJ, Fail PS, Smalling RW, Siegel R, Rose GA, Engeron E, Loghin C, Trento A, Skipper ER, Fudge T, Letsou GV, Massaro JM, Mauri L, For the EVEREST II Investigators: Percutaneous Repair or Surgery for Mitral Regurgitation. New Engl J Med 364:1395-1406, 2011.
- Whitlow P, Feldman T, Pedersen W, Lim S, Kipperman R, Smalling R, Bajwa T, Herrmann H, Lasala J, Kramer P, Maddux J, Tuzcu M, Kapadia S, Trento A, Siegel, R, Foster E, Glower D. The EVEREST II High Risk Study: Acute and 12 Month Results with Catheter Based Mitral Valve Leaflet Repair. J Am Coll Cardiol 59: 130-139, 2012.
- Lim DS, Reynolds MR, Feldman T, Kar S, Herrmann HC, Wang A, Whitlow PL, Gray WA, Grayburn P, Mack MJ, Glower D: Improved Functional Status and Quality of Life in Prohibitive Surgical Risk Patients With Degenerative Mitral Regurgitation Following Transcatheter Mitral Valve Repair with the MitraClip System. J Am Coll Cardiol. 2013 Oct 24. pii: S0735-1097(13)05864-6. doi: 10.1016/j.jacc.2013.10.021. [Epub ahead of print]
- Feldman T, Young A: Percutaneous Approaches to Valve Repair for Mitral Regurgitation. J Am Coll Cardiol (2014), doi: 10.1016/j.jacc.2014.01.039.
Clinical Topics: Cardiac Surgery, Invasive Cardiovascular Angiography and Intervention, Valvular Heart Disease, Cardiac Surgery and VHD, Interventions and Structural Heart Disease, Mitral Regurgitation
Keywords: Cardiac Surgical Procedures, Heart Valve Prosthesis Implantation, Mitral Valve, Mitral Valve Insufficiency
< Back to Listings