Left Atrial Appendage Exclusion Devices – Where Are They Going?
Cardioembolic stroke is the most severe consequence of atrial fibrillation (AF) and is increased 4-5 fold in patients with AF. The annual risk of cardioembolic stroke increases sharply with age, as does the risk of severe bleeding complicating oral anticoagulation (OAC) therapy.1
The inherent challenges and consequences with the use of OAC therapy for stroke prevention in AF has led to the development of alternative methods for stroke prevention such as left atrial appendage (LAA) closure. Surgical closure of the LAA was first proposed in the 1940’s, based on an observation that the LAA was a potential site of thrombus. A more recent analysis found that in 91% of patients with non-rheumatic AF and 57% with rheumatic AF, left atrial thrombi were isolated to or originated from the LAA.2 As a prophylactic measure during mitral valve procedures, suture ligation from the endocardial surface of the left atrium is often performed as recommended in the AHA/ACC guidelines for the management of patients with valvular heart disease.3 Percutaneous LAA implant devices were initially developed as alternatives to surgical closure of the LAA. The demonstration of non-inferiority in the PROTECT AF trial of the LAA implant compared to warfarin provided the proof of concept that exclusion of the LAA is beneficial in preventing cardioembolic events and bleeding consequences related to OAC therapy.4 This has led to the development of both endocardial and epicardial approaches for the exclusion of the LAA. Endocardial implants are perceived as being easier to use, while epicardial approaches do not leave a foreign body in the LAA. Which device or approach for exclusion of the LAA is dependent upon morphology and size of the LAA, but ultimately will be based on efficacy of LAA closure and complication rates.
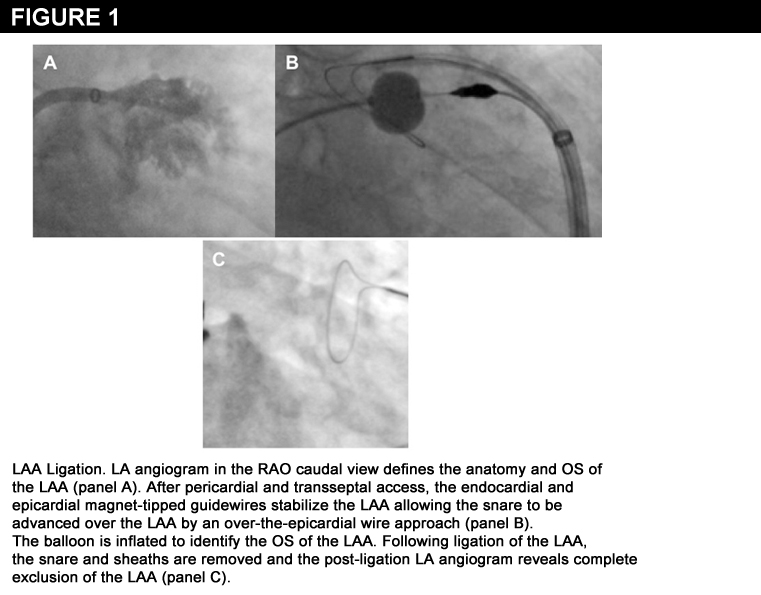 The LAA implant device used in the PROTECT AF trial has become the prototype for LAA implants due to the vast clinical experience and trial data. Recently, a catheter-based LAA ligation procedure has been developed using an epicardial approach.5 Pericardial and transseptal access is used to connect an endocardial magnet-tipped guidewire to an epicardial magnet-tipped guidewire to stabilize the LAA (Figure 1). The suture delivery device consists of a snare with a pre-tied suture that is advanced over the LAA by an over-the-epicardial wire approach. Once the suture delivery device is positioned over the LAA, the snare is closed, suture released, knot tightened, remnant suture cut and the suture delivery device is removed resulting in complete closure of the LAA without a foreign body. LAA ligation with the suture delivery device has been shown to produce a LAA complete closure rate of 96%, no device complications and an acceptably low access related complication rate.5
The LAA implant device used in the PROTECT AF trial has become the prototype for LAA implants due to the vast clinical experience and trial data. Recently, a catheter-based LAA ligation procedure has been developed using an epicardial approach.5 Pericardial and transseptal access is used to connect an endocardial magnet-tipped guidewire to an epicardial magnet-tipped guidewire to stabilize the LAA (Figure 1). The suture delivery device consists of a snare with a pre-tied suture that is advanced over the LAA by an over-the-epicardial wire approach. Once the suture delivery device is positioned over the LAA, the snare is closed, suture released, knot tightened, remnant suture cut and the suture delivery device is removed resulting in complete closure of the LAA without a foreign body. LAA ligation with the suture delivery device has been shown to produce a LAA complete closure rate of 96%, no device complications and an acceptably low access related complication rate.5
With the development of effective LAA closure devices, is there a rationale for LAA exclusion during AF ablation? The HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation states that decisions regarding the use of warfarin more than two months following ablation should be based on the patient’s risk factors for stroke and not on the presence or type of AF.6 Discontinuation of warfarin therapy post ablation is generally not recommended in patients who have a CHADS score > 2. Therefore, the concomitant exclusion of the LAA during or following pulmonary vein isolation (PVI) for the treatment of AF would provide a strategy of performing AF ablation for the treatment of symptoms related to AF and exclusion of the LAA for the prevention of thrombus formation in the LAA, thus providing an alternative to long-term OAC therapy post-PVI. With the results of the Protect AF study demonstrating non-inferiority to warfarin therapy, one could consider PVI with implantation of an LAA implant device. After two months of warfarin therapy post-PVI and LAA device implantation, discontinuation of warfarin could be considered.
The left atrial appendage has been suggested to be an under recognized trigger site of AF.7 This has lead to the strategy of ablation of the LAA to create electrical isolation. However, complete LAA electrical isolation can lead to LAA mechanical standstill resulting in thrombus formation. Therefore, exclusion of the LAA following electrical isolation of the LAA seems prudent. In addition to LAA implants, epicardial approaches can be used for LAA exclusion. A potential advantage of epicardial LAA exclusion is the resultant LAA electrical isolation without the need for ablation. LAA exclusion with clips have demonstrated LAA electrical isolation. Han et al. recently reported that LAA ligation with the suture delivery device significantly attenuates LAA electrical activity with complete abolition of LAA electrical activity in over 30% of patients once the snare is closed.8 Therefore, complete tightening of the suture should result in complete electrical isolation for the LAA in addition to complete LAA closure.
An appealing use of LAA ligation with the suture delivery device is the potential to perform a closed chested MAZE procedure. A pilot study at the University of California, San Francisco has demonstrated feasibility of concomitant LAA ligation and PVI. Additional studies are needed to determine whether LAA ligation may also improve AF ablation outcomes.
References
- Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomized controlled trials. Arch Intern Med 1994;154:1449-57.
- Blackshear JL, Odell JA. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann Thorac Surg 1996;61:755-759.
- ACC/AHA guidelines for the management of patients with valvular heart disease. A report of the American College of Cardiology/American Heart Association. Task Force on Practice Guidelines (Committee on Management of Patients with Valvular Heart Disease). J Am Coll Cardiol 1998; 32:1486-588.
- Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, Mullin CM, Sick P. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet 2009;374:534-542.
- Bartus K, Han F, Bednarek J, Myc J, Kapelak B, Sadowski J, Lelakowski J, Yakubov SJ, Lee RJ. Percutaneous Left Atrial Appendage Suture Ligation Using the LARIAT in Patients with Atrial Fibrillation: Initial Clinical Experience. J Am Coll Cardiol 2012 (In press, available on line).
- The HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation. Heart Rhythm 2007;6:816-61.
- Di Biase L, Burkhardt JD, Mohanty P, et al.Left Atrial Appendage : An Underrecognized Trigger Site of Atrial Fibrillation. Circulation 2010;122:109-118.
- Han FT, Bartus K, Bednarek J, Badhwar N, Lee RJ. Electrical isolation of the LAA occurs following epicardial LAA ligation. Abstract presented at Cardiostim, Nice, France 2012.
Clinical Topics: Anticoagulation Management, Arrhythmias and Clinical EP, Anticoagulation Management and Atrial Fibrillation, Atrial Fibrillation/Supraventricular Arrhythmias
Keywords: Atrial Appendage, Atrial Fibrillation, Ligation, Mitral Valve, Risk Factors, San Francisco, Stroke, Warfarin
< Back to Listings