Which CV Patients Suffering From Sleep Apnea May Be Candidates for Surgical Treatment?
 Mr. Jones is a 72-year-old new patient in your practice with HTN, high cholesterol, and a strong family history of coronary artery disease. He recently moved to your area with his wife to be closer to their six grandchildren. During the initial visit he describes an active life without chest pain, exercise intolerance, or shortness of breath. Coronary calcium scoring, treadmill stress test, and carotid IMT were all normal. His cholesterol is well controlled. He is a non-smoker. His Epworth score indicates daytime fatigue at nine, and his wife reports loud snoring and frequent breath-holding episodes. Your eight-person cardiology group actively screens for sleep disordered breathing and routinely performs overnight polysomnography when indicated, as there is plethora of data linking cardiovascular disease to sleep apnea. Mr. Jones is identified to have obstructive sleep apnea Syndrome (OSAS) and is started on continuous positive airway pressure (CPAP) therapy. At your follow-up visit in three months, he has lost 25 pounds, developed nasal congestion, and has a large node in his left neck. You send him to an otolaryngologist who diagnoses a stage IV nasopharyngeal squamous cell carcinoma.
Mr. Jones is a 72-year-old new patient in your practice with HTN, high cholesterol, and a strong family history of coronary artery disease. He recently moved to your area with his wife to be closer to their six grandchildren. During the initial visit he describes an active life without chest pain, exercise intolerance, or shortness of breath. Coronary calcium scoring, treadmill stress test, and carotid IMT were all normal. His cholesterol is well controlled. He is a non-smoker. His Epworth score indicates daytime fatigue at nine, and his wife reports loud snoring and frequent breath-holding episodes. Your eight-person cardiology group actively screens for sleep disordered breathing and routinely performs overnight polysomnography when indicated, as there is plethora of data linking cardiovascular disease to sleep apnea. Mr. Jones is identified to have obstructive sleep apnea Syndrome (OSAS) and is started on continuous positive airway pressure (CPAP) therapy. At your follow-up visit in three months, he has lost 25 pounds, developed nasal congestion, and has a large node in his left neck. You send him to an otolaryngologist who diagnoses a stage IV nasopharyngeal squamous cell carcinoma.
This vignette illustrates one of the pitfalls encountered when treating sleep disordered breathing, that is, the failure to pick up an upper airway mass as the cause for a patient's obstructive symptoms. Who needs to see an otolaryngologist? How do I avoid the situation described above? Should I even be involved in diagnostic sleep medicine?
Given the myriad of associations between apnea and cardiovascular disease, cardiologists have to be involved with the diagnosis and treatment of sleep apnea. It is as important as checking cholesterol levels, treating HTN, and performing a good heart and vascular exam. Simple modifications to the exam and history can help to avoid delays in diagnosis and help to triage patients into the appropriate arm of treatment (positive pressure therapy, upper airway surgery, or oral appliance).
Screening for Patients at Risk for OSAS
Traditionally, subjective questionnaires aimed at assessing daytime sleepiness have been the screening tool for sleep disordered breathing. The Epworth sleepiness scale is the most commonly used tool in the outpatient setting. Other tools such as the STOP-BANG assessment have proven useful in prospective trials in stratifying perioperative risk with regards to sleep apnea but have not been validated in the outpatient setting.1
 Many studies have demonstrated the poor predictive value of the Epworth score, particularly in older patients such as those typically seen in a cardiology practice.2 Likewise, the use of objective physical parameters alone, such as neck circumference or body mass index, is equally problematic in cardiovascular patients. Because of this lack of sensitivity in any single screening tool and the high prevalence of both central and obstructive sleep disordered breathing in patients with cardiovascular disease, it is important that the cardiologist have a low threshold for sleep apnea testing. The less expensive home testing modalities make a lower positive test rate more acceptable, particularly given the negative impact unrecognized sleep apnea can have on cardiovascular disease.
Many studies have demonstrated the poor predictive value of the Epworth score, particularly in older patients such as those typically seen in a cardiology practice.2 Likewise, the use of objective physical parameters alone, such as neck circumference or body mass index, is equally problematic in cardiovascular patients. Because of this lack of sensitivity in any single screening tool and the high prevalence of both central and obstructive sleep disordered breathing in patients with cardiovascular disease, it is important that the cardiologist have a low threshold for sleep apnea testing. The less expensive home testing modalities make a lower positive test rate more acceptable, particularly given the negative impact unrecognized sleep apnea can have on cardiovascular disease.
Cardiologists should consider sleep apnea testing in any patient with cardiovascular disease known to be associated with sleep disordered breathing. These include heart failure, arrhythmia, known coronary disease, refractory multidrug hypertension, patients with coronary stents, and the metabolic syndrome.3
OSAS and the Physical Exam – Cardiology Style
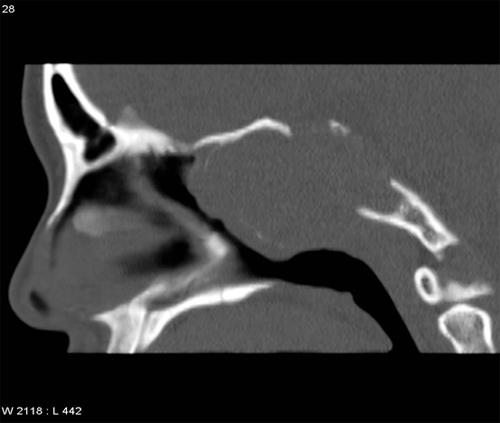
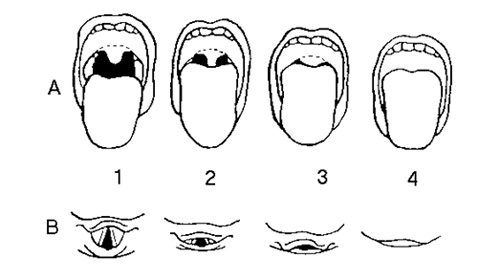 The physical exam is also very important in identifying patients at risk for sleep disorders. While 80% of sleep apnea patients have a BMI greater than 30, the remaining 20% are not obese. The cause for the apnea in 90% of non-obese patients is due to abnormal bony facial development.4 This is easily picked up on a quick exam of the facial profile and oral cavity. Patients with retrognathia, a modified Mallampati score of 3 or 4, or evidence of lateral growth retardation of the maxilla (high arched palate, narrow dental arch) should be considered at high risk for sleep apnea.
The physical exam is also very important in identifying patients at risk for sleep disorders. While 80% of sleep apnea patients have a BMI greater than 30, the remaining 20% are not obese. The cause for the apnea in 90% of non-obese patients is due to abnormal bony facial development.4 This is easily picked up on a quick exam of the facial profile and oral cavity. Patients with retrognathia, a modified Mallampati score of 3 or 4, or evidence of lateral growth retardation of the maxilla (high arched palate, narrow dental arch) should be considered at high risk for sleep apnea.
Who Needs to See ENT?
This is best broken down into two groups. The first group would be patients with some risk factor for neoplastic disease. As presented in the case study, upper airway masses in the nasopharynx, larynx, or hypopharynx can have positive sleep studies due to the obstructive effect of the neoplasm on the airway. Clues in the history, physical exam, or sleep study results themselves that should raise the cardiologist's index of suspicion for neoplastic disease are listed below:
History
Smoking or heavy alcohol use
Hemoptysis, throat pain, or dysphagia
Unexplained weight loss
New sudden onset heroic snoring
Positional dyspnea
History of upper airway neoplasm
Globus sensation
Physical Exam
Hoarseness
Neck mass or thyroid goiter
Cranial nerve findings
Tonsillar asymmetry
Sleep Testing and Treatment Results
Marked differences in AHI depending on body position
Severe AHI without significant hypoxia
Increasing CPAP pressure requirements over time without weight gain
Choking with use of CPAP
Surgery Anyone?
Patients also suitable for ENT evaluation are those who may be candidates for surgery as a primary curative treatment option or as a way to improve CPAP compliance. Studies clearly show that nasal surgery in patients with moderate to severe nasal congestion can promote CPAP compliance.5 While full-faced masks are an option, many patients prefer nasal only mask interfaces, making an adequate nasal airway a necessity. Patients with a deviated septum, marked allergic disease, severe turbinate hypertrophy, and those with severe nasal congestion all should be sent to ENT for a surgical evaluation.
The question of which patients are appropriate surgical candidates as primary treatment for their apnea is hotly debated. Medicine has done a poor job of determining which patients may benefit from surgery while refusing surgery to those who are poor candidates. A patient's anatomy determines whether they are a good candidate for surgery, and not their weight, age, or severity of AHI. Sleep apnea surgery is designed to increase the diameter of the upper airway while making its dynamic segments less collapsible. As a general rule, patients with marked bony abnormalities outlined above (mandibular or maxillary hypoplasia) are not good candidates for soft tissue surgery of the upper airway. If the underlying facial skeletal structure is abnormal or underdeveloped, soft tissue surgery should be deferred. In those cases, consideration should be given to an oral surgery consult for bony maxillofacial surgery.
If the skeletal anatomy exhibits normal development, attention should be turned to the soft tissue elements of the airway. Close attention should be paid towards the size and relationship of the tonsils and tongue. In general, patients with smaller tongues and larger tonsils are better candidates for upper airway surgery. The relationship between the two is best assessed with the modified Mallampati score. Patients with scores of one or two indicate a small tongue relative to the palate and generally are better candidates for palatal surgery. It is important to note that even patients with Mallampati scores of three or four can make good surgical candidates but generally require multi-level surgery to include resection of the base of tongue in addition to the palatal procedure.
The most important thing for the cardiologist to develop is a relationship with a trusted ear, nose and throat (ENT) specialist specifically trained in sleep apnea surgery. Traditional surgical options such as the uvulopalatopharyngoplasty (UPPP) are falling out of favor and being replaced with functional palatal procedures such as palatal advancement procedures and expansion sphincter pharyngoplasties.6 These, in combination with base of tongue resections, have been shown to have markedly increased cure rates as compared to more traditional soft tissue apnea procedures such as UPPP. The author's experience with these newer multilevel procedures yields surgical cure rates of 85-90% as defined by a 50% reduction in AHI in combination with an absolute number less than 20. Woodson's published data cited above shows similar surgical cure rates with these procedures performed in the right patients.
In summary, cardiologists MUST play an active role in identifying and treating patients with OSAS. The incorporation of several very simple questions into the patient's history coupled with a quick facial assessment, nasal exam, and oral cavity exam can help determine which patients need to be seen by an otolaryngologist for an endoscopic exam or possibly surgical treatment of their disease.
References
- Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008;108:812-21.
- Sil A, Barr G. Assessment of predictive ability of Epworth scoring in screening of patients with sleep apnoea. J Laryngol Otol 2012;126:372-9.
- Quan SF, Howard BV, Iber C, et al. The Sleep Heart Health Study: design, rationale, and methods. Sleep 1997;20:1077-85.
- Sakakibara H, Tong M, Matsushita K, Hirata M, Konishi Y, Suetsugu S. Cephalometric abnormalities in non-obese and obese patients with obstructive sleep apnoea. Eur Respir J 1999;13:403-10.
- Chandrashekariah R, Shaman Z, Auckley D. Impact of upper airway surgery on CPAP compliance in difficult-to-manage obstructive sleep apnea. Arch Otolaryngol Head Neck Surg 2008;134:926-30.
- Pang KP, Woodson BT. Expansion sphincter pharyngoplasty: a new technique for the treatment of obstructive sleep apnea. Otolaryngol Head Neck Surg 2007;137:110-4.
Clinical Topics: Heart Failure and Cardiomyopathies, Sleep Apnea
Keywords: Sleep Apnea Syndromes, Cardiovascular Diseases
< Back to Listings