Pericoronary Adipose Tissue Inflammation on Coronary CT in Patients With Vasospastic Angina
Quick Takes
- Coronary spasm may be associated with pericoronary adipose tissue inflammation represented by computed tomography angiography (CTA) derived right coronary artery (RCA) pericoronary adipose tissue attenuation index.
- Fat attenuation index assessment of the inner and thinner 2-mm pericoronary adipose tissue may provide better diagnostic performance for vasospastic angina than the standard method for fat attenuation index assessment.
Introduction
Coronary artery spasm plays an important role in the pathogenesis of not only chronic coronary artery disease, such as vasospastic angina, but also myocardial infarction. Ohyama et al. examined fluorine-18-labeled (18F) fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) scans and showed that levels of perivascular inflammation were higher in patients with vasospasm than in those without.1 They also demonstrated that coronary perivascular FDG uptake showed a significant positive correlation with optical coherence tomography-defined extent of vasa vasorum formation in coronary adventitial layer. This finding may suggest that CTA could provide information related to the inflammation of the inner layer of pericoronary adipose tissue by virtue of its higher resolution compared with PET/CT, which is limited by low availability, high cost, and the requirement of a radioactive tracer. The study examined whether vasospastic angina is associated with pericoronary adipose tissue inflammation as represented by CTA-derived fat attenuation index. Furthermore, it examined whether assessment of the inner pericoronary adipose tissue layer might be superior for diagnosis of vasospastic angina compared with the previously reported method.2
Study Design and Patient Population
This post hoc analysis was performed in patients undergoing spasm provocation test with intracoronary acetylcholine (Ach) at Tsuchiura Kyodo General Hospital between May 2015 and August 2019. Patients undergoing CTA before spasm provocation test were selected from the institutional registry of patients with suspected vasospastic angina undergoing spasm provocation test. The final study population consisted of 88 patients undergoing CTA with sufficient image quality and spasm provocation test.
Coronary Angiography, Spasm Provocation Test, and Diagnosis of Vasospastic Angina
Spasm provocation test with intracoronary Ach injection was performed in accordance with the guidelines of the Japanese Circulation Society.3 Angiographic coronary artery vasospasm was defined as induction of total or subtotal occlusion during spasm provocation test. A positive diagnosis was made when angiographic coronary artery vasospasm accompanied by chest pain and/or ischemic electrocardiographic changes, such as transient ST-segment elevation ≥0.1 mV, ST-segment depression ≥0.1 mV, or new appearance of negative U waves, recorded in at least 2 contiguous leads on the 12-lead electrocardiogram according to the guidelines.3
CTA Protocol and Pericoronary Inflammation Assessment
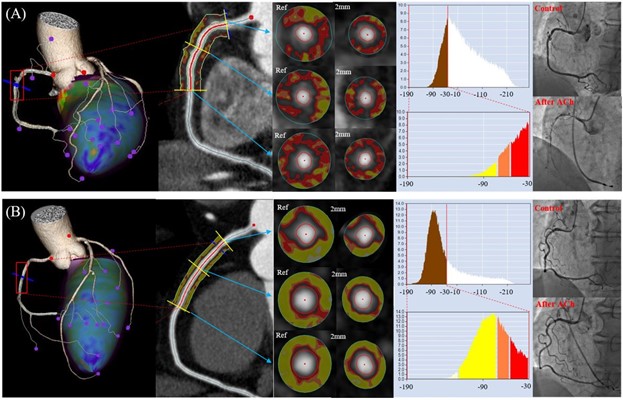
Cardiac CTA was performed with a 320-row scanner (Aquilion ONE [Toshiba Medical Systems; Otawara, Japan]) within 1 month before the spasm provocation test in all patients. In the study, analyses were performed of pericoronary adipose tissue attenuation values on CTA of all 3 main coronary vessels. Fat attenuation index analysis was performed using a dedicated workstation (Aquarius iNtuition Edition version 4.4.13 [TeraRecon Inc.; Foster City, CA]).2 Fat attenuation index was evaluated for the proximal reference diameter (reference fat attenuation index) and inner 2-mm adipose tissue layer (2-mm fat attenuation index) from the vessel wall for 40 mm in length (Figure 1). The mean fat attenuation index values of 3 major coronary arteries of both reference fat attenuation index and 2-mm fat attenuation index were obtained and compared between vasospastic angina and non-vasospastic angina groups.
Figure 1
Results
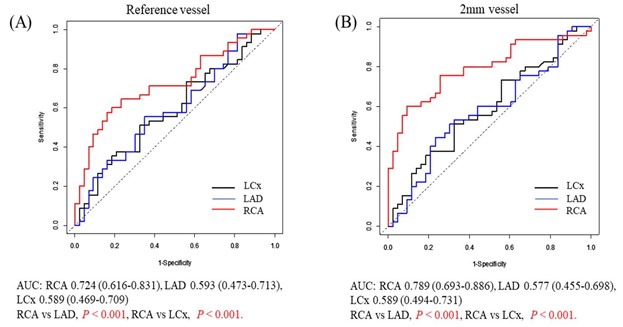
A diagnosis of vasospastic angina was made in 45 patients (51.1% of vasospastic angina group). There were no significant differences in baseline characteristics between the vasospastic angina and non-vasospastic angina groups. Figure 1 shows 2 representative cases from the vasospastic angina and non-vasospastic angina groups. In the vasospastic angina group, RCA 2-mm fat attenuation index and RCA reference fat attenuation index (diameter 3.4 ± 0.8 mm) both showed significantly higher fat attenuation index values than those in the non-vasospastic angina group. Of note, both RCA reference fat attenuation index and RCA 2-mm fat attenuation index showed significantly better diagnostic performance than fat attenuation index values obtained from left anterior descending (LAD) and left circumflex artery (LCx) (Figure 2). Furthermore, RCA 2-mm fat attenuation index showed significantly better diagnostic performance for predicting vasospastic angina than RCA reference fat attenuation index. When limiting the analysis to the patients with RCA spasm (n = 26), RCA 2-mm fat attenuation index showed better performance for predicting vasospastic angina compared with RCA reference fat attenuation index.
Figure 2
Predictors of Vasospastic Angina
The results of univariable and multivariable logistic regression analyses to predict vasospastic angina diagnosis are shown in Table 1. Multivariable analysis revealed that the independent predictors of vasospastic angina were hypertension (odds ratio [OR] 3.29, 1.11-9.69; p = 0.031) and RCA 2-mm fat attenuation index (OR 1.17, 1.08-1.27; p < 0.001). ROC analysis revealed that the best cut-off value of RCA 2-mm fat attenuation index to predict vasospastic angina was -62.3 (area under the curve [AUC] 0.789, 0.693-0.886; p < 0.001)
Table 1: Logistic Regression Analysis for Predicting Vasospastic Angina
| Univariable Analysis | Multivariable Analysis | |||||
| OR | 95% confidence interval | P value | OR | 95% confidence interval | P value | |
| Age | 0.998 | 0.97-1.03 | 0.911 | |||
| Male | 2.43 | 0.953-6.19 | 0.063 | 1.07 | 0.345-3.33 | 0.904 |
| Smoker | 1.21 | 0.490-2.99 | 0.678 | |||
| Estimated glomerular filtration rate | 1.00 | 0.976-1.03 | 0.989 | |||
| C-reactive protein | 3.24 | 0.498-21.0 | 0.219 | |||
| Hypertension | 2.41 | 0.988-5.86 | 0.053 | 3.29 | 1.11-9.69 | 0.031 |
| Aspirin | 2.65 | 0.758-9.25 | 0.127 | |||
| Beta-blocker | 6.40 | 0.745-56.1 | 0.091 | 6.88 | 0.530-89.4 | 0.140 |
| RCA 2-mm fat attenuation index | 1.16 | 1.08-1.24 | <0.001 | 1.177 | 1.08-1.27 | <0.001 |
Discussion
The study was performed to investigate the association between fat attenuation index values obtained by CTA and diagnosis of vasospastic angina by spasm provocation test according to the clinical guidelines.3 The main findings of this study follow:
- In patients with vasospastic angina, fat attenuation index values obtained by routine CTA were significantly higher than those in patients without vasospastic angina.
- RCA fat attenuation index values showed significantly better diagnostic efficacy for predicting vasospastic angina compared to left coronary artery fat attenuation index.
- RCA 2-mm fat attenuation index, which corresponds to the inner adipose tissue assessment close to the vessel wall, compared with RCA reference fat attenuation index values obtained by the previously reported method showed better discriminating efficacy for vasospastic angina diagnosis.
- Hypertension and RCA 2-mm fat attenuation index were independent and significant predictors of vasospastic angina diagnosis.
Association Between Pericoronary Adipose Tissue Inflammation and Coronary Vasospasm
Fat attenuation index assessed by the inner adipose tissue of 2-mm thickness from the outer coronary artery wall is associated with better diagnostic efficacy compared with the method reported by Antonopoulos et al.5 Recent advances in translational research using noninvasive imaging modalities, including 18F-FDG PET and CTA, have enabled us to visualize perivascular inflammation in the pathogenesis of coronary artery spasm. The results of the study are in line with the report by Antonopoulos et al.5 that suggested the link between pericoronary gradient of lipid accumulation and a shift from a greater to a lesser lipophilic content closer to the vessel wall. These results are also concordant with the findings by Ohyama and Shimokawa, who showed that coronary perivascular FDG uptake was positively correlated with those of adventitial vasa vasorum formation on optical coherence tomography.1
Clinical Implications
Comprehensive assessment including CT fat attenuation index mapping of pericoronary adipose tissue may offer a novel tool for quantifying adipose tissue inflammation and detecting the potential of vasospastic angina without no additional contrast, cost, and radiation or tracers over anatomical assessment.
Conclusion
CTA-derived fat attenuation index was significantly higher in patients with vasospastic angina, suggesting an important link between coronary spasm and pericoronary adipose tissue inflammation, particularly with adventitia and perivascular adipose tissue close to the coronary wall.
References
- Ohyama K, Matsumoto Y, Takanami K, et al. Coronary Adventitial and Perivascular Adipose Tissue Inflammation in Patients With Vasospastic Angina. J Am Coll Cardiol 2018;71:414-25.
- Oikonomou EK, Marwan M, Desai MY, et al. Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data. Lancet 2018;392:929-39.
- JCS Joint Working Group. Guidelines for diagnosis and treatment of patients with vasospastic angina (Coronary Spastic Angina) (JCS 2013). Circ J 2014;78:2779-801.
- Ueno H, Hoshino M, Sugiyama T, et al. Pericoronary Adipose Tissue Inflammation on Coronary Computed Tomography in Patients With Vasospastic Angina. JACC Cardiovasc Imaging 2021;14:511-2.
- Antonopoulos AS, Sanna F, Sabharwal N, et al. Detecting human coronary inflammation by imaging perivascular fat. Sci Transl Med 2017;9:eaal2658.
Clinical Topics: Cardiovascular Care Team, Invasive Cardiovascular Angiography and Intervention, Noninvasive Imaging, Prevention, Stable Ischemic Heart Disease, Atherosclerotic Disease (CAD/PAD), Interventions and Coronary Artery Disease, Interventions and Imaging, Angiography, Nuclear Imaging, Hypertension, Chronic Angina
Keywords: Diagnostic Imaging, Fluorodeoxyglucose F18, Coronary Vasospasm, Acetylcholine, Fluorine, Coronary Angiography, Vasa Vasorum, Tomography, Optical Coherence, Coronary Artery Disease, Area Under Curve, Radioactive Tracers, ROC Curve, Hospitals, General, Logistic Models, Chest Pain, Electrocardiography, Myocardial Infarction, Hypertension, Registries, Inflammation, Spasm, Adipose Tissue
< Back to Listings