2023 ESH Hypertension Guideline Update: Bringing Us Closer Together Across the Pond
Quick Takes
- The 2023 European Society of Hypertension (ESH) and 2017 American College of Cardiology/American Heart Association (ACC/AHA) hypertension guidelines both emphasize proper blood pressure (BP) measurement, cardiovascular (CV) risk assessment, optimal lifestyle interventions, and specific pharmacotherapy management.
- Both guidelines recommend a lower BP target (<130/80 mm Hg) for adults at high risk to reduce the risk of CV events.
- Key differences include a lower diagnostic threshold by ACC/AHA criteria (<130/80 mm Hg) than by ESH criteria (<140/90 mm Hg) and age-based treatment targets (ESH criteria).
Introduction
Hypertension represents a major modifiable risk factor for coronary artery disease (CAD), heart failure (HF), stroke, chronic kidney disease (CKD), and dementia.1 Two well-established clinical practice guidelines on hypertension include the 2017 American College of Cardiology/American Heart Association (ACC/AHA) Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults and the recently published 2023 European Society of Hypertension (ESH) Guidelines for the Management of Arterial Hypertension.2,3 This analysis reviews key similarities and differences between these guidelines.
Importance of Accurate Blood Pressure Measurement
Both guidelines stress the importance of standardized, accurate measurement of blood pressure (BP) and recommend office-based measurements for diagnosis. Although both agree that validated, cuffed devices should be used for BP measurements, the ESH guidelines explicitly recommend against use of cuffless measurement devices. The ESH guidelines point to a lack of standardized validation protocols to test the accuracy of these devices and list concerns about the need for periodic calibration and use of novel predictive technologies to estimate BP.4,5 There is consensus that multiple office BP measurements and BP tracking with either home BP monitoring or ambulatory BP monitoring should be performed before diagnosing hypertension. Compared with the 2018 European Society of Cardiology (ESC)/ESH Guidelines for the Management of Arterial Hypertension, the 2023 ESH guidelines emphasize using out-of-office BP monitoring in addition to traditional in-office measurements to diagnose hypertension.6
Cardiovascular Risk Stratification
Both guidelines recommend cardiovascular disease (CVD) risk assessment. The ESH guidelines recommend using the updated Systematic Coronary Risk Evaluation 2 (SCORE2) tool for CVD risk stratification.7 This risk-estimation model is derived from data from a large cohort of Europeans without clinical CVD or diabetes mellitus (DM).7 Whereas the original Systematic Coronary Risk Evaluation (SCORE) tool included only fatal CVD events, the SCORE2 tool estimates 10-year risk of both fatal and nonfatal CVD events in adults 40-69 years of age, which aligns with the CVD risk assessment tool recommended by the ACC/AHA guideline.2 The ACC/AHA guideline recommends using the Pooled Cohort Equation (PCE) to estimate 10-year risk of fatal and nonfatal CVD events in adults 40-79 years of age.2 Unlike the ACC/AHA guideline, the ESH guidelines recommend using a separate risk assessment tool for adults ≥70 years of age, derived from a large Norwegian cohort: the Systematic Coronary Risk Evaluation 2–Older Persons (SCORE2-OP).8 Whereas the PCE is used to guide treatment decisions of hypertension, the SCORE2 is not. The ACC/AHA guideline recommends calculating risk in primary-prevention patients and starting medical therapy at a lower BP threshold for patients at high risk.
Blood Pressure Categories and Hypertension Diagnosis
The 2023 ESH guidelines maintain the same BP grade classifications as the 2018 ESC/ESH guidelines.6 The ESH recommends a threshold of >140/90 mm Hg (grade 1) for the diagnosis of hypertension, whereas the ACC/AHA guideline recommends a lower threshold of >130/80 mm Hg (stage 1). Systolic blood pressure (SBP) ranging between 130 and 139 mm Hg or diastolic blood pressure (DBP) ranging between 80 and 89 mm Hg represent stage 1 hypertension in the ACC/AHA guideline, whereas the ESH guidelines classify these ranges as "normal" or "high-normal" (130-139/85-89 mm Hg). Whereas the ACC/AHA guideline categorizes BP ≥140/90 mm Hg as stage 2 hypertension, the ESH guidelines subdivide BP levels ≥140/90 mm Hg into grades 1, 2, and 3 hypertension (Table 1).
Table 1: Similarities and Differences Between ACC/AHA and ESH Guidelines on Hypertension
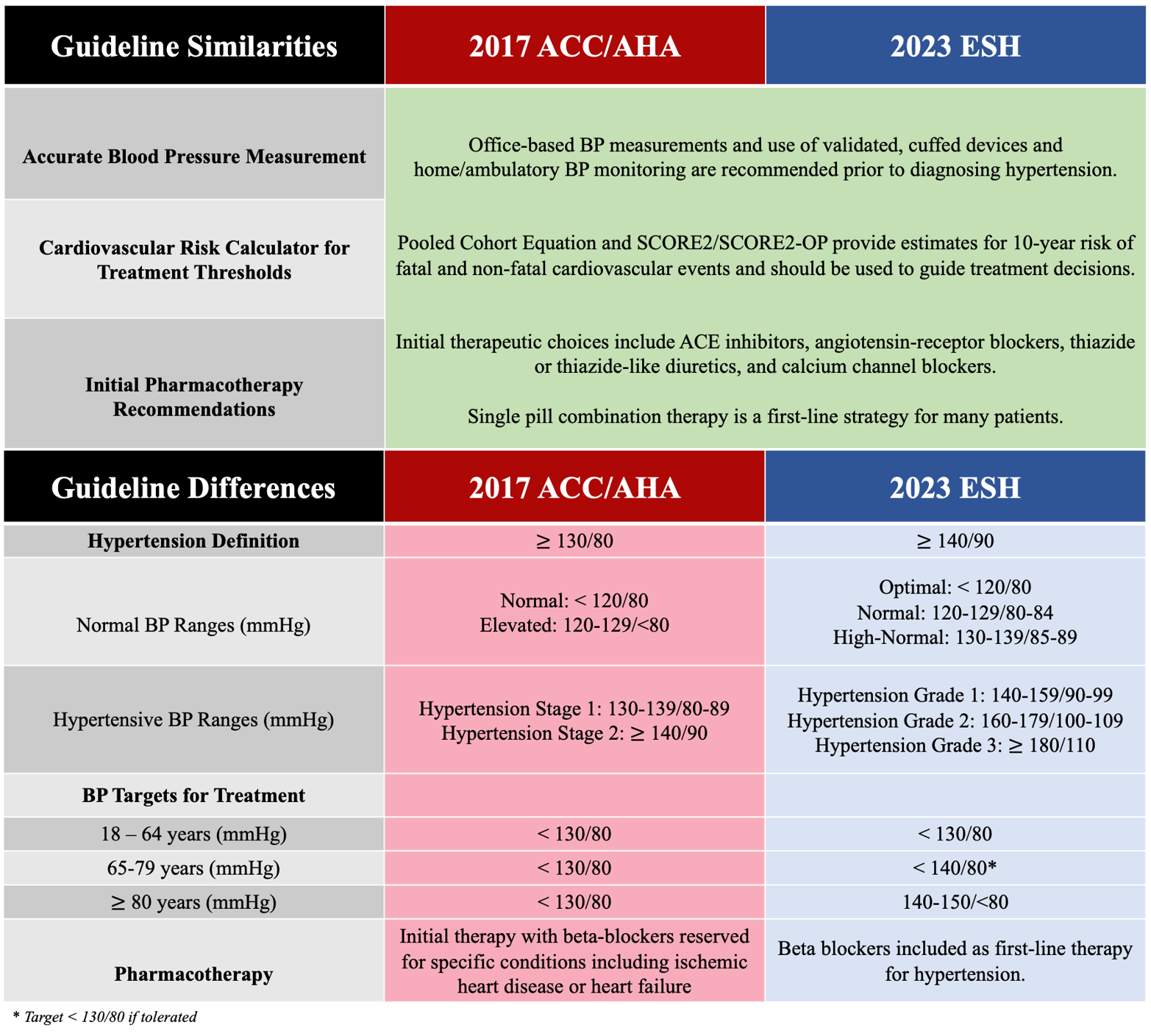
ACC = American College of Cardiology; ACE = angiotensin-converting enzyme; AHA = American Heart Association; BP = blood pressure; ESH = European Society of Hypertension; SCORE2 = Systematic Coronary Risk Evaluation 2; SCORE2-OP = Systematic Coronary Risk Evaluation 2–Older Persons.
Blood Pressure Treatment Targets
The ACC/AHA guideline recommends treatment to a BP target of <130/80 mm Hg for many patients. The ESH guidelines recommend BP treatment targets that differ on the basis of age. Although the ESH guidelines recommend the same BP treatment target as the ACC/AHA guideline for many adults, the ESH guidelines recommend higher BP treatment thresholds for adults >65 years of age. The ESH guidelines target BP <140/80 mm Hg for patients 65-79 years of age. For patients in this age group with isolated systolic hypertension and for adults ≥80 years of age, the threshold is even more lenient, targeting SBP between 140 and 150 mm Hg. The ESH guidelines also recommend a higher BP target (<140/90 mm Hg) for patients with hypertension and CKD than does the ACC/AHA guideline (<130/80 mm Hg), but recommend the same BP target (<130/80 mm Hg) for patients with hypertension and coexisting CAD, DM, and cerebrovascular disease.
Recommendations for Drug Therapy Initiation
Promotion of lifestyle interventions to prevent, treat, and delay onset of hypertension feature prominently in both guidelines.2,3 Both guidelines recommend treatment initiation with antihypertensive agents for patients who have established CVD and BP ≥130/80 mm Hg. The ACC/AHA guideline further specifies that patients who have an estimated 10-year risk of atherosclerotic CVD of >10% should also be started on treatment. Both guidelines recommend treatment initiation at higher BP thresholds of SBP ≥140 mm Hg and/or DBP ≥90 mm Hg regardless of calculated cardiovascular (CV) risk or established CVD. For older adults (>80 years of age), the ESH guidelines explicitly recommend drug therapy when SBP is >160 mm Hg, whereas the ACC/AHA guideline does not make this distinction.
Pharmacotherapy
Both guidelines recommend that initial therapies include at least one of four major classes: angiotensin-converting enzyme inhibitors (ACEIs), angiotensin-receptor blockers (ARBs), thiazide or thiazide-like diuretics, and calcium channel blockers (CCBs). The ESH guidelines continue to include beta-blockers (BBs) as an optional first-line therapy on the basis of randomized controlled trial evidence, whereas the ACC/AHA guideline does not. The guidelines both emphasize use of BBs for patients with a history of ischemic heart disease or HF. The ESH guidelines also recommend consideration of BBs in the treatment of other CV and non-CV conditions, such as atrial fibrillation, hypertension in pregnancy, and hyperthyroidism.9
Both guidelines recommend single-pill combination therapy to reduce pill burden and improve adherence. The ESH guidelines recommend the preferred combination of ACEIs or ARBs with either CCBs or thiazide/thiazide-like diuretics. Whereas the ESH guidelines strongly emphasize initial treatment with a two-drug combination for most patients with hypertension, the ACC/AHA guideline recommends this approach for patients with stage 2 hypertension, those with BP >20/10 mm Hg above their target BP, and Black patients.
Renal Denervation Therapy
The updated ESH guidelines now recommend consideration of renal denervation therapy as an additional or alternative therapy in patients who have uncontrolled resistant hypertension or adverse effects to medications, which is a change from the 2018 ESC/ESH guidelines.3
Conclusions
The 2023 ESH guidelines did not endorse major changes to their primary recommendations; however, the guidelines now align more closely with the 2017 ACC/AHA guideline. Although these guidelines represent a step toward guideline harmonization, key differences remain, including when to initiate therapy.
References
- Fuchs FD, Whelton PK. High blood pressure and cardiovascular disease. Hypertension 2020;75:285-92.
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APha/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018;71:e127-e248.
- Mancia G, Kreutz R, Brunström M, et al. 2023 ESH guidelines for the management of arterial hypertension the Task Force for the management of arterial hypertension of the European Society of Hypertension: endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens 2023;41:1874-2071.
- Stergiou GS, Mukkamala R, Avolio A, et al.; European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability. Cuffless blood pressure measuring devices: review and statement by the European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability. J Hypertens 2022;40:1449-60.
- Mukkamala R, Yavarimanesh M, Natarajan K, et al. (2021). Evaluation of the accuracy of cuffless blood pressure measurement devices: challenges and proposals. Hypertension 2021;78:1161-7.
- Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens 2018;36:1953-2041.
- SCORE2 Working Group and ESC Cardiovascular Risk Collaboration. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. Eur Heart J 2021;42:2439-54.
- SCORE2-OP Working Group and ESC Cardiovascular Risk Collaboration. SCORE2-OP risk prediction algorithms: estimating incident cardiovascular event risk in older persons in four geographical risk regions. Eur Heart J 2021;42:2455-67.
- Mancia G, Kjeldsen SE, Kreutz R, Pathak A, Grassi G, Esler M. Individualized beta-blocker treatment for high blood pressure dictated by medical comorbidities: indications beyond the 2018 European Society of Cardiology/European Society of Hypertension guidelines. Hypertension 2022;79:1153-66.
Clinical Topics: Prevention, Hypertension
Keywords: Blood Pressure, Blood Pressure Monitors, Hypertension, Primary Prevention, Secondary Prevention, Cardiovascular Diseases
< Back to Listings