Benefit of Fractional Flow Reserve Assessment of Intermediate Coronary Lesions in TAVI
Quick Takes
- The most appropriate management of coronary artery disease in transcatheter aortic valve implantation (TAVI) candidates is still debated.
- The FAITAVI (Functional Assessment In TAVI) trial investigators assessed the prognostic impact of fractional flow reserve (FFR) coronary lesion physiology compared with angiography-guided revascularization in stable TAVI patients with intermediate coronary lesions.
- FFR-guided percutaneous coronary intervention reduced major adverse cardiovascular events, especially overall mortality and ischemia-driven target-vessel revascularization, without increasing the risk of bleeding.
Over 50% of patients with aortic stenosis (AS) have concomitant coronary artery disease (CAD).1 The most appropriate management of CAD before transcatheter aortic valve implantation (TAVI) is still debated, with contrasting indications provided by European and American guidelines: the European guidelines favor percutaneous coronary intervention (PCI) over a combined surgical approach for revascularization and the American guidelines for valve disease correction.2-3 Physiologic guidance for PCI has been demonstrated to improve outcomes compared with angiography alone; however, the feasibility and reliability of functional assessment of coronary stenoses in patients with severe AS has been largely questioned. Recent studies have suggested that fractional flow reserve (FFR) is less affected by valve disease than other nonhyperemic indexes,4 although underestimation of CAD severity could not be completely excluded.5 The NOTION-3 (Third Nordic Aortic Valve Intervention) trial previously demonstrated that, in TAVI candidates with at least one physiologically significant coronary lesion amenable to PCI, the combination of percutaneous revascularization followed by aortic valve correction reduced the risk of death, myocardial infarction (MI), and urgent revascularization compared with TAVI alone.6
The FAITAVI (Functional Assessment In TAVI) randomized trial aimed to assess whether FFR-guided management improves clinical outcomes compared with angiography-guided revascularization in stable TAVI patients with coronary lesions ≥50% (Figure 1). Three hundred and twenty patients were enrolled in 15 Italian centers, with a mean age of 86 years and low SYNTAX (Synergy Between Percutaneous Coronary Intervention With TAXUS and Cardiac Surgery) score (median 7) being similar between the two groups.7 PCI was performed prior to TAVI only in approximately 40% of patients and scheduled within 1 month after valve replacement in 24% of patients in both groups. Revascularization and TAVI were performed in the same procedure in approximately one-third of the sample after valve implantation in 18% of patients in the FFR-guided arm and in 24% of patients in the angiography-guided arm. The 12-month follow-up results, recently presented at EuroPCR 2025 in Paris, France, showed that the primary endpoint of major adverse cardiac and cerebrovascular events occurred in 14 patients (8.5%) in the FFR-guided PCI group and in 25 patients (16%) in the angiography-guided PCI group (p = 0.047). In particular, overall mortality and ischemia-driven target-vessel revascularization showed the greatest reduction, with no safety concern in terms of major bleeding, acute kidney failure, periprocedural MI, and vascular complications in the PCI group.8
Figure 1: FAITAVI Trial Design and Select Findings
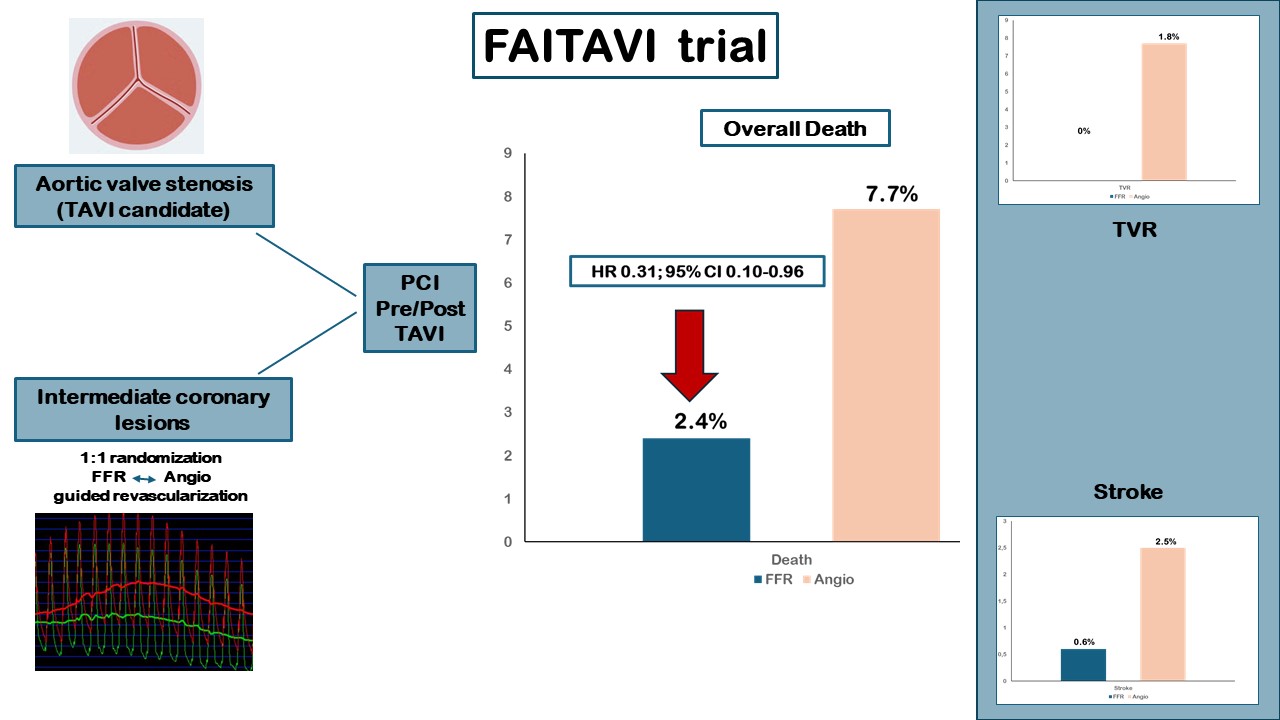
Angio = angiography; CI = confidence interval; FAITAVI = Functional Assessment In TAVI; FFR = fractional flow reserve; HR = hazard ratio; TAVI = transcatheter aortic valve intervention; TVR = target-vessel revascularization.
Data from the FAITAVI trial confirm comparable prognostic benefits of FFR for guiding PCI in patients with and without severe AS, significantly impacting clinical decision-making when dealing with bystander CAD in patients who are candidates for TAVI. The investigators acknowledged several limitations constraining the generalizability of the study, including the small number of participants and enrollment in a single European country. Moreover, a medical therapy arm was not included in this trial. Patients underwent coronary revascularization only after valve replacement. The most appropriate timing of PCI in TAVI candidates is a consideration. A recent meta-analysis including 1,531 patients with stable CAD showed a reduction in mortality when PCI was performed after rather than before TAVI (5.8% vs. 20.1%; p = 0.02).9 However, the total number of patients managed with this strategy was modest; thus, larger-scale, dedicated studies would better refine the indications and criteria for tailoring the approach to patients with CAD and AS requiring TAVI, a very complex population at high risk whose appropriate management has been underexplored.
References
- Tarantini G, Tang G, Nai Fovino L, et al. Management of coronary artery disease in patients undergoing transcatheter aortic valve implantation. A clinical consensus statement from the European Association of Percutaneous Cardiovascular Interventions in collaboration with the ESC Working Group on Cardiovascular Surgery. EuroIntervention. 2023;19(1):37-52. doi:10.4244/EIJ-D-22-00958
- Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. EuroIntervention. 2022;17(14):e1126-e1196. Published 2022 Feb 4. doi:10.4244/EIJ-E-21-00009
- Writing Committee Members, Otto CM, Nishimura RA, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol. 2021 Feb 2;77(4):509. doi: 10.1016/j.jacc.2020.12.040.] [published correction appears in J Am Coll Cardiol. 2021 Mar 9;77(9):1275. doi: 10.1016/j.jacc.2021.02.007.] [published correction appears in J Am Coll Cardiol. 2023 Aug 29;82(9):969. doi: 10.1016/j.jacc.2023.07.010.] [published correction appears in J Am Coll Cardiol. 2024 Oct 29;84(18):1772. doi: 10.1016/j.jacc.2024.09.025.]. J Am Coll Cardiol. 2021;77(4):e25-e197. doi:10.1016/j.jacc.2020.11.018
- Jo HH, Kang DY, Lee JM, et al. Evaluation of instantaneous wave-free ratio and fractional flow reserve in severe aortic valve stenosis. Circ Cardiovasc Interv. 2024;17(5):e013237. doi:10.1161/CIRCINTERVENTIONS.123.013237
- Minten L, McCutcheon K, Vanhaverbeke M, et al. Coronary physiological indexes to evaluate myocardial ischemia in patients with aortic stenosis undergoing valve replacement. JACC Cardiovasc Interv. 2025;18(2):201-212. doi:10.1016/j.jcin.2024.10.024
- Lønborg J, Jabbari R, Sabbah M, et al. PCI in patients undergoing transcatheter aortic-valve implantation. N Engl J Med. 2024;391(23):2189-2200. doi:10.1056/NEJMoa2401513
- Ribichini F, Pesarini G, Fabris T, et al. A randomised multicentre study of angiography- versus physiology-guided percutaneous coronary intervention in patients with coronary artery disease undergoing TAVI: design and rationale of the FAITAVI trial. EuroIntervention. 2024;20(8):e504-e510. Published 2024 Apr 15. doi:10.4244/EIJ-D-23-00679
- Ribichini F. Angiography versus physiology-guided PCI in patients undergoing TAVI: the functional assessment in TAVI (FAITAVI) trial. Presented at EuroPCR 2025, Paris, France. May 21, 2025.
- Caminiti R, Ielasi A, Vetta G, et al. Percutaneous coronary intervention before or after transcatheter aortic valve replacement: a systematic review and meta-analysis involving 1531 patients. J Clin Med. 2024;13(12):3521. Published 2024 Jun 16. doi:10.3390/jcm13123521
Clinical Topics: Cardiac Surgery, Invasive Cardiovascular Angiography and Intervention, Aortic Surgery, Stable Ischemic Heart Disease, Valvular Heart Disease
Keywords: Fractional Flow Reserve, Myocardial, Transcatheter Aortic Valve Replacement, Percutaneous Coronary Intervention