PURE: Secondary Prevention Medications For CVD Underused Globally
Secondary prevention medications for cardiovascular diseases are underused globally and additional strategies to increase their use are needed to improve management and reduce premature mortality rates, according to results from the PURE study published in JACC.
The landmark multinational, community-based study observed more than 11,000 participants with diagnosed cardiovascular disease from 17 countries over a median follow-up of 12 years. Median age at baseline was 58 years, and 52.9% of participants were female. Participating countries, arranged by World Bank income classification, included:
- High-income: Canada, Sweden, United Arab Emirates
- Upper-middle-income: Argentina, Brazil, Chile, Malaysia, Poland, South Africa, Türkiye
- Lower-middle-income: China, Colombia, Iran
- Low-income: Bangladesh, India, Pakistan, Zimbabwe
Researchers looked at medication use for participants with coronary artery disease (antiplatelet agents, statins, renin-angiotensin-system (RAS) inhibitors and beta-blockers) and with stroke (antiplatelet agents, statins, RAS inhibitors and other blood pressure-lowering drugs). Medications were collected at baseline and four subsequent follow-up visits. Overall findings showed that medication use for secondary cardiovascular disease prevention varied by country income level and was lower at the last study visit compared to the first visit in every income level except for upper-middle-income countries.
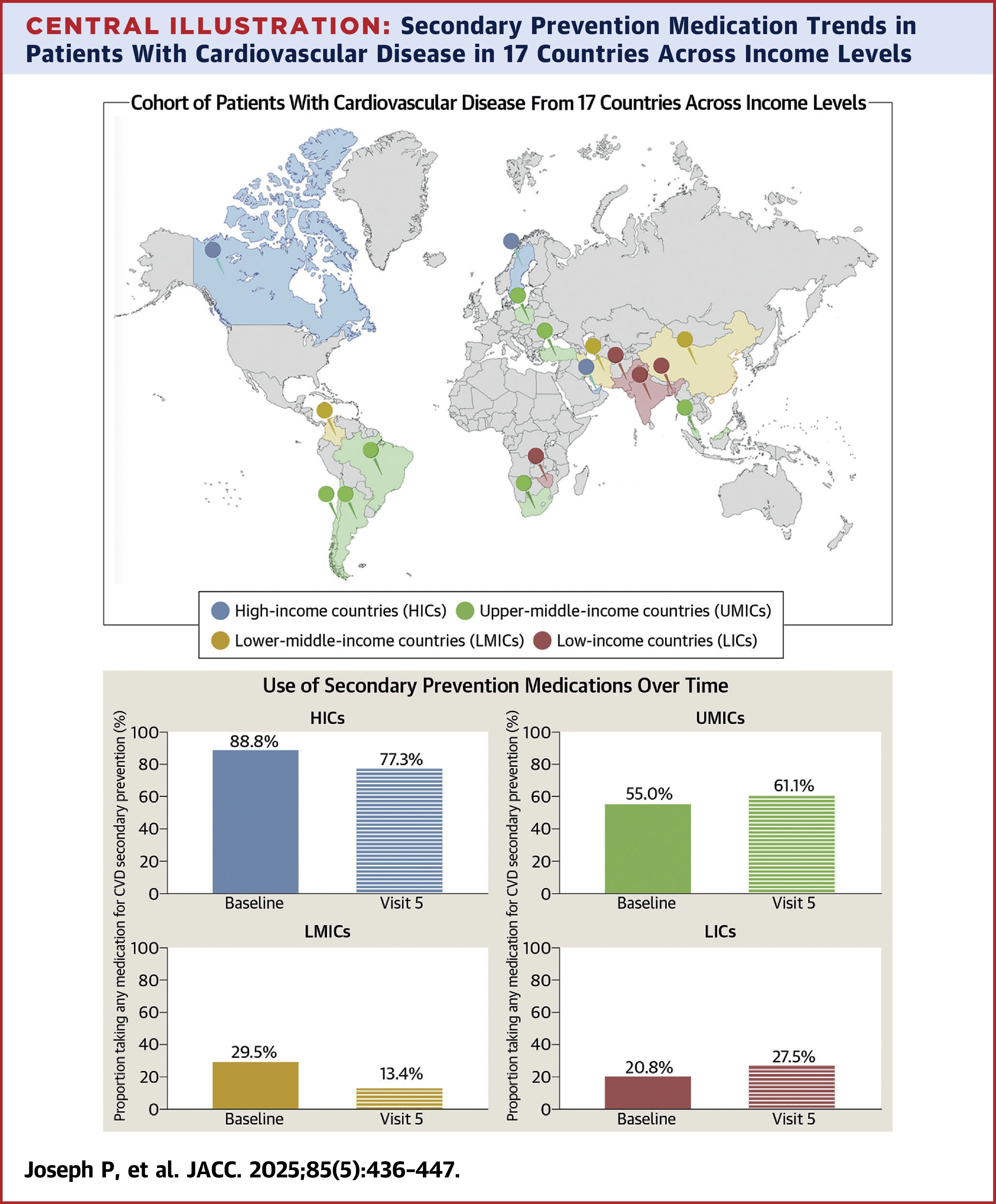
Overall, the use of at least one medication for secondary prevention started at 41.3% at the baseline study visit, peaked at 43.1%, and dropped to 31.3% at the last study visit. In high-income countries, use declined from 88.8% to 77.3%. In upper-middle-income countries, it rose from 55% to 61.1%. In lower-middle-income countries, it began at 29.5%, peaked at 31.7%, and fell to 13.4%. In low-income countries, it increased from 20.8% to a peak of 47.3%, then declined to 27.5%. Use of three or more proven medication classes for secondary prevention was substantially lower in all country income levels.
"Our findings suggest that current secondary prevention strategies continue to leave the majority of people with [cardiovascular disease] either untreated or undertreated and highlight the general lack of progress being made to increase the use of secondary [cardiovascular disease} prevention medications in most parts of the world," said Philip Joseph, MD, FACC, lead author of the study and scientist at the Population Health Research Institute.
While the PURE analysis is largely descriptive, Joseph and colleagues note their findings are important in that they "highlight the general lack of progress being made to increase the use of secondary cardiovascular disease prevention medications in most parts of the world," despite the World Health Organization's Global Action Plan and focused United Nations Sustainable Developmental Goals. "Outside of setting targets and issuing guidelines, there have been few systematic implementation efforts to increase the uptake of secondary [cardiovascular disease] prevention medications in most countries, and new strategies are needed," they write.
JACC Editor-in-Chief Harlan M. Krumholz, MD, SM, FACC, underscores the need for new strategies and the immense opportunity to improve global cardiovascular health. "It is unacceptable that so many individuals worldwide who have already experienced heart disease are not receiving readily available and inexpensive treatments that could save lives and prevent further events. We have the tools to bridge this gap in care now – and we must act urgently," he says.
In a related editorial comment, Oyere K. Onuma, MD, FACC, writes that "the use of novel and innovative strategies must be a key lynchpin in solving the secondary prevention conundrum" and also stresses the need for urgent action to address the rural-urban divide crisis. "The key to closing the gap for secondary prevention lies in supporting an implementation-science perspective, with a focus on locally adapted strategies coupled with an audacious and bold global campaign for achieving this target of scaling up secondary prevention efforts globally," Onuma says.
In another editorial comment, Abhishek Chaturvedi, MD, and Dorairaj Prabhakaran, MD, suggest that actions must be "community-based, patient-centered, incorporate social determinants of health, and involve task-sharing with nonphysician health care workers." The highlight the use of polypills, cost-effective digital health options, on-the-job training programs, and continued collaborations among global cardiovascular societies to bridge knowledge gaps and generate localized data, as examples of strategies that can move the needle.
Clinical Topics: Dyslipidemia, Atherosclerotic Disease (CAD/PAD), Nonstatins, Novel Agents, Statins
Keywords: Coronary Artery Disease, Blood Pressure, Hydroxymethylglutaryl-CoA Reductase Inhibitors, ACC International, Stroke
< Back to Listings