
Is Aficamten Plus Disopyramide More Effective Than Aficamten Alone in oHCM?
The addition of aficamten to disopyramide was effective and well-tolerated in patients with symptomatic obstructive hypertrophic cardiomyopathy (oHCM) with persistent left ventricular overflow tract (LVOT) obstruction, and the withdrawal of disopyramide did not reduce the effectiveness of aficamten, according to research published May 7 in JACC: Heart Failure.
Ahmad Masri, MD, FACC, et al., drew from three trials of patients with oHCM: the open-label REDWOOD-HCM Cohort 3, the placebo-controlled SEQUOIA-HCM and the open-label FOREST-HCM. They identified 50 unique patients (mean age 58-63 years, 46% women, 88% White), resulting in 93 subjects (segments) with persistent symptomatic oHCM despite disopyramide treatment across four groups: 1) disopyramide plus aficamten and subsequent aficamten withdrawal (n=29); 2) disopyramide plus placebo (n=20); 3) aficamten plus disopyramide and subsequent disopyramide withdrawal (n=17); and 4) continued both disopyramide and aficamten (n=27). The mean disopyramide dose across the four groups was 331 mg/d.
Among all patients, 90% were receiving a beta-blocker and 12% a calcium-channel blocker; 38% had NYHA functional class III severe symptoms. Mean LVEF ranged from 68%-70%, mean resting LVOT gradient from 50-64 mm Hg and mean Valsalva LVOT gradient from 87-94 mm Hg. Both NT-proBNP and high-sensitivity troponin I (hsTnI) were abnormally elevated in all four groups.
Results showed that adding aficamten to disopyramide improved LVOT obstruction (least squares mean [LSM] change at rest –27.0 mm Hg and on Valsava –39.2 (p<0.0001 for both). Furthermore, it alleviated symptoms, with NYHA functional class improving by one or more in 78% of patients and Kansas City Cardiomyopathy Questionnaire-Clinical Summary Score (KCCQ-CSS) improving by 12.3 points. The NT-proBNP ratio was reduced by 0.35 and hsTnI by 0.74.
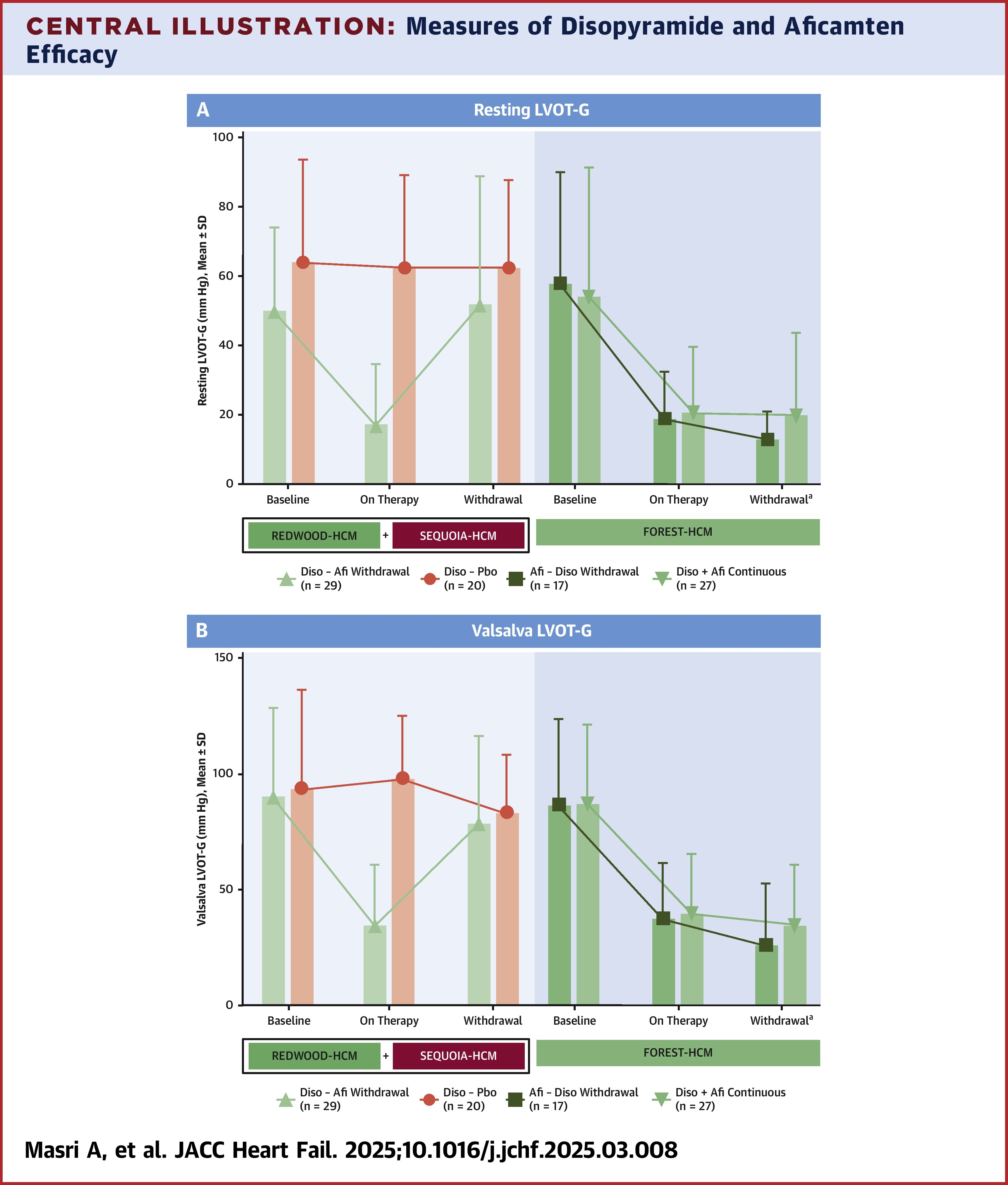
In contrast, in patients taking disopyramide, withdrawing aficamten led to a return of LVOT obstruction (LSM change in resting LVOT gradient 44.1 mm Hg and Valsalva 65.5 mm Hg; p<0.0001 for both), as well as worsening of symptoms and an increase in NT-proBNP to baseline levels. Of note, however, there was no loss of efficacy when withdrawing aficamten.
Among patients in the aficamten plus disopyramide plus disopyramide withdrawal group, adding aficamten significantly improved NHYA function class in 82% of patients compared with 74% among patients who continued both drugs. In both groups, aficamten significantly improved KCCQ-CSS (LSM change 10.4 and 16.1 respectively). Moreover, the improvement in hemodynamics gained with aficamten were not lost when disopyramide was withdrawn, nor was there any worsening in NHYA class or KCCQ-CSS or effect on NT-proBNP, although there was a gradual reduction in hsTnI in patients who continued on disopyramide.
Among the patients who continued on both disopyramide and aficamten, no differences were observed in hemodynamics or biomarkers, but worsening of symptoms was observed with prolonged use of disopyramide.
No safety events were associated with withdrawing either drug and no atrial fibrillation was observed after withdrawing disopyramide.
The authors note that while disopyramide has been prescribed for patients for more than four decades, risk of tachyphylaxis and anticholinergic side effects can limit its use. They also note the "tendency for physicians to add, rather than replace, therapies for LVOT obstruction."
"Because nearly all the clinically relevant outcome measures obtained from patients who were withdrawn from disopyramide remained stable, but improved with aficamten monotherapy, these data support the emerging treatment principle that disopyramide may not provide additional clinical benefit in patients who are concurrently treated with aficamten," write the authors. "However, given the relatively small sample size, additional studies should be considered to confirm these initial observations.
Clinical Topics: Heart Failure and Cardiomyopathies, Acute Heart Failure
Keywords: Cardiomyopathy, Hypertrophic, Hypertrophic Cardiomyopathy, Heart Failure, Ventricular Outflow Obstruction, Disopyramide
< Back to Listings