CVD Risk in Cancer Survivors Varies By Cancer Type and Treatment
The long-term risk of cardiovascular disease (CVD) among cancer survivors can vary significantly based on cancer type and treatment, according to a nationwide cohort study published June 17 in JACC: CardioOncology.
Using data from Danish health care registries, Frits I. Mulder, MD, et al., identified 91,407 adult cancer survivors (mean age 67 years; 63% women) who received systemic cancer treatment and were free of treatment three years after diagnosis. They compared the survivors with 457,035 age- and sex-matched cancer-free individuals from the general population.
The most common cancer types among survivors were breast in 44%, prostate in 15% and colorectal in 13%. Regarding the type of cancer treatment, 63% received chemotherapy in the first 12 months after diagnosis. Other treatments included alkylating agents in 22%, antimetabolites in 17%, cytotoxic antibiotics in 20%, plant alkaloids in 25% or platinum compounds in 17%.
Five-year results showed that cancer survivors vs. matched individuals had an increased risk of heart failure or cardiomyopathy (hazard ratio [HR], 1.08); venous thromboembolism (VTE) (HR, 1.50); pericarditis, endocarditis or myocarditis (HR, 1.30); and kidney failure (HR, 1.17). No increased risk was seen for ischemic heart disease, stroke or atrial fibrillation.
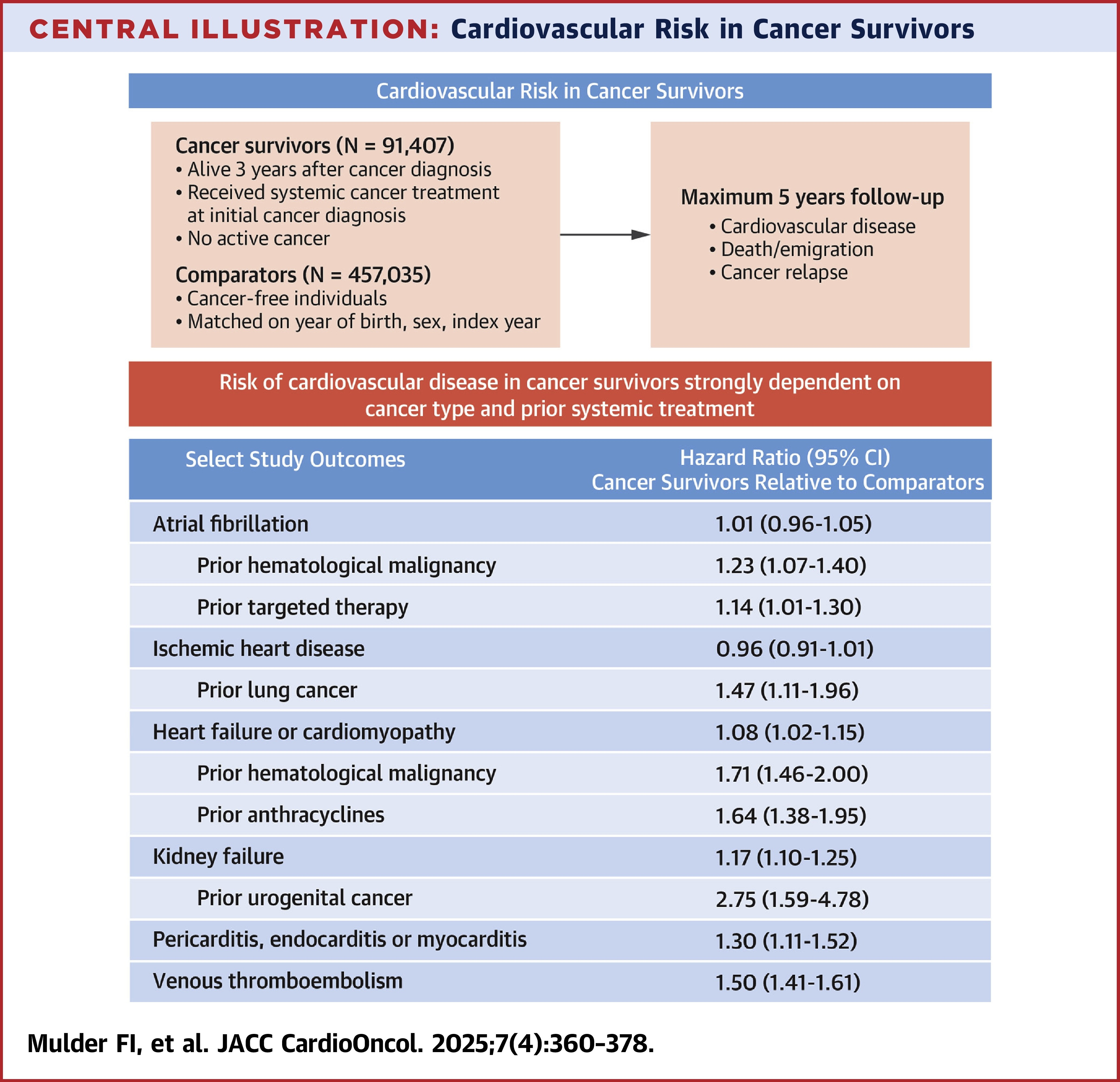
In terms of cardiovascular events by cancer type and treatment, estimates varied considerably. For instance, the risk of VTE was higher across all treatment groups and all cancer types except gastrointestinal, while the risk of ischemic heart disease was higher only in lung cancer survivors. No increased risk of hypertension was observed. Regarding treatment agents, stroke was associated only with platinum compounds.
"Given the considerable variation in risk across subgroups," Mulder and colleagues advise that "monitoring strategies should follow a personalized, risk-based approach."
In an accompanying editorial comment, Nina Nouhravesh, MD, and Morten Schou, MD, write that the study results "challenge the prevailing assumption that universal [cardiovascular] screening is warranted for the majority of cancer survivors. Given the vast and growing size of the survivor population, such an approach is neither feasible nor likely justifiable. Instead, the data strongly support a more targeted strategy, indicating that a subset of patients is likely to benefit from structured surveillance programs."
Clinical Topics: Arrhythmias and Clinical EP, Cardiovascular Care Team, Heart Failure and Cardiomyopathies, Pulmonary Hypertension and Venous Thromboembolism, Vascular Medicine, Implantable Devices, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Acute Heart Failure
Keywords: Cancer Survivors, Venous Thromboembolism, Myocardial Infarction, Arrhythmias, Cardiac, Cardiac Arrhythmias, Heart Failure, Stroke, Renal Insufficiency, Neoplasms
< Back to Listings