PRAGUE-25: What Is the Best Intervention Strategy For AFib In Obesity?
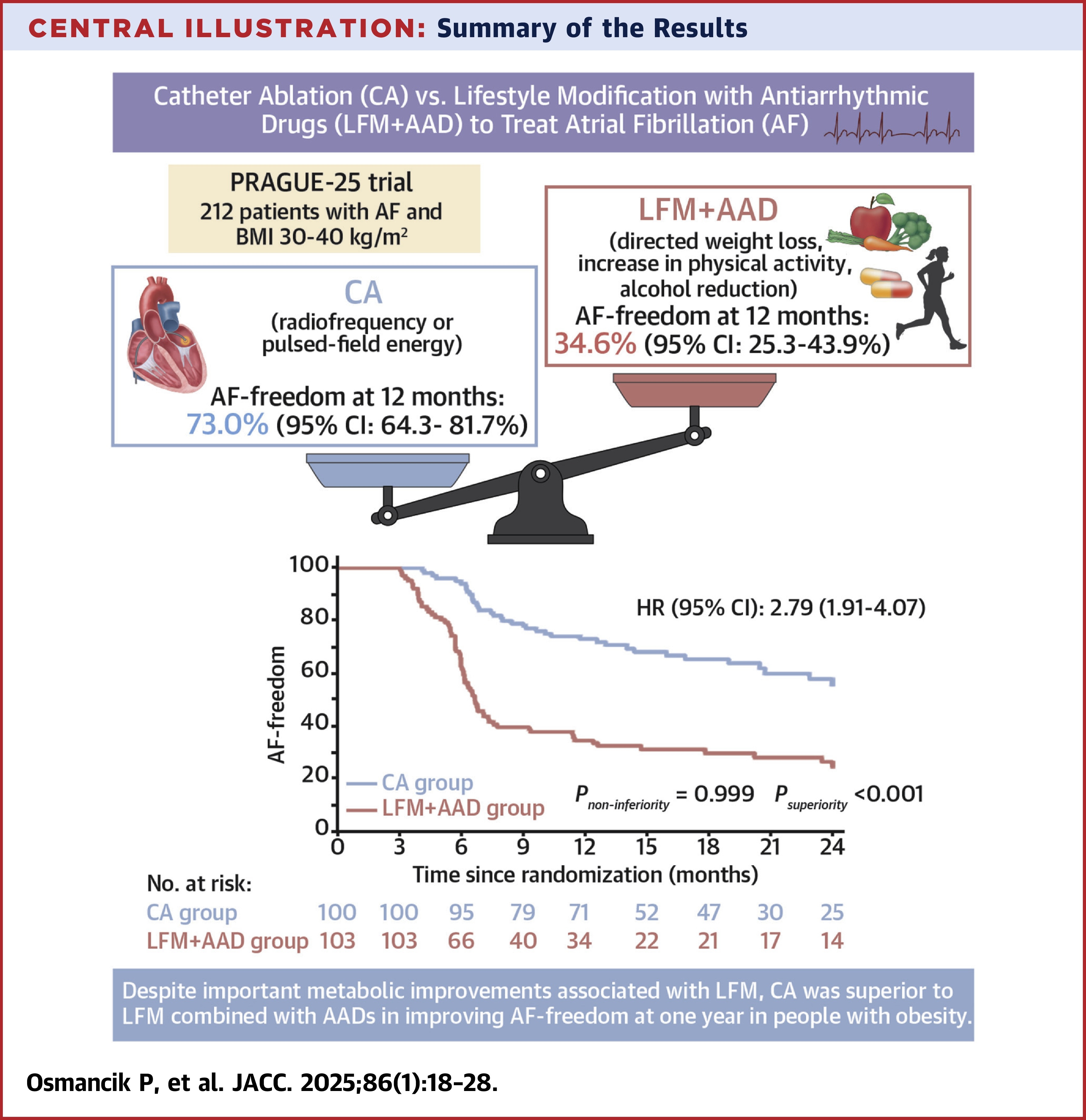
Catheter ablation (CA) was superior to a combination of lifestyle modification (LFM) and antiarrhythmic drugs (AADs) in improving freedom from atrial fibrillation (AFib) at one year in patients with obesity, according to results from the PRAGUE-25 trial published in JACC.
In the multicenter noninferiority PRAGUE-25 trial, Pavel Osmancik, MD, PhD, et al., randomized 203 patients (median age 60; 32% women) in the Czech Republic with either paroxysmal AFib (56%) or persistent/long-standing persistent AFib (44%) and a BMI) of 30-40 kg/m2 (average BMI 34.9 kg/m2) to either CA (n=100) or LFM+AAD (n=103). During the trial, 26 patients crossed over treatment groups (all but one from LFM+AAD to CA) but only three occurred before the primary endpoint had been reached.
LFM consisted of consultations with nutritional specialists and physiotherapists, who guided patients in recording calorie intake, decreasing alcohol consumption and following individual exercise programs. AAD selection was left to physician discretion.
The primary endpoint was AFib freedom, defined as an absence of any AFib episode lasting more than 30 seconds. It was evaluated by seven-day Holter recordings taken every three months, electrocardiograms taken during outpatient visits and documented AFib at unplanned patient visits. Mean follow-up was 23.5 months, following a three-month blanking period after randomization.
Results showed that at one year, 73% of patients in the CA arm maintained AFib freedom vs. 35% in the LFM+AAD arm (hazard ratio, 2.79; pnoninferiority =0.99 and psuperiority <0.001).
Clinically relevant major complications occurred in one patient in the CA arm (1%) who experienced a transitory ischemic attack, and four in the LFM+AAD arm (3.8%), with three experiencing syncope and one experiencing sudden cardiac death.
The authors note that despite CA's superiority, both weight change (–6.4 kg vs. –0.35 kg; p<0.001) and decreased HbA1c were more significant in the LFM+AAD group. "Patients with obesity should not be discouraged from losing weight, because several other significant benefits are associated with weight reduction," they write. Nonetheless, "the referral to CA in this population should not be delayed until the patient loses weight."
"There is no question that [CA] is superior to AAD therapy for the prevention of recurrent atrial arrhythmia as demonstrated unequivocally in this trial," write Ratika Parkash, MD, MSc, and Jonathan Piccini, MD, MHS, FACC, in an accompanying editorial comment, "but the effect of LFM and its benefits cannot be minimized."
"The most important question is what overall clinical strategy provides the greatest net clinical benefit," they continue. "The data from this trial and others strongly suggest that the optimal treatment strategy is [CA] paired with LFM. The impact of LFM remains integral to improving longer-term outcomes in patients with [AFib], including those who are treated with [CA]."
Clinical Topics: Arrhythmias and Clinical EP, EP Basic Science, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias
Keywords: Atrial Fibrillation, Anti-Arrhythmia Agents, Obesity, Catheter Ablation
< Back to Listings