New Concise Clinical Guidance Addresses Evaluation and Management of ATTR-CM
A new ACC Concise Clinical Guidance (CCG) report on "Transthyretin Cardiac Amyloidosis Evaluation and Management" provides updated strategies and best practices for clinicians, taking into account expanding disease modifying therapies, heart failure (HF) therapies and potential future opportunities.
The CCG summarizes four key challenges associated with the diagnosis, evaluation and management of transthyretin amyloid cardiomyopathy (ATTR-CM), which is increasingly recognized as a cause of HF particularly in older individuals. These challenges include a high index of suspicion, conducting an appropriate diagnostic evaluation, the need for an individualized management strategy and awareness of unanswered questions based on evolving evidence.
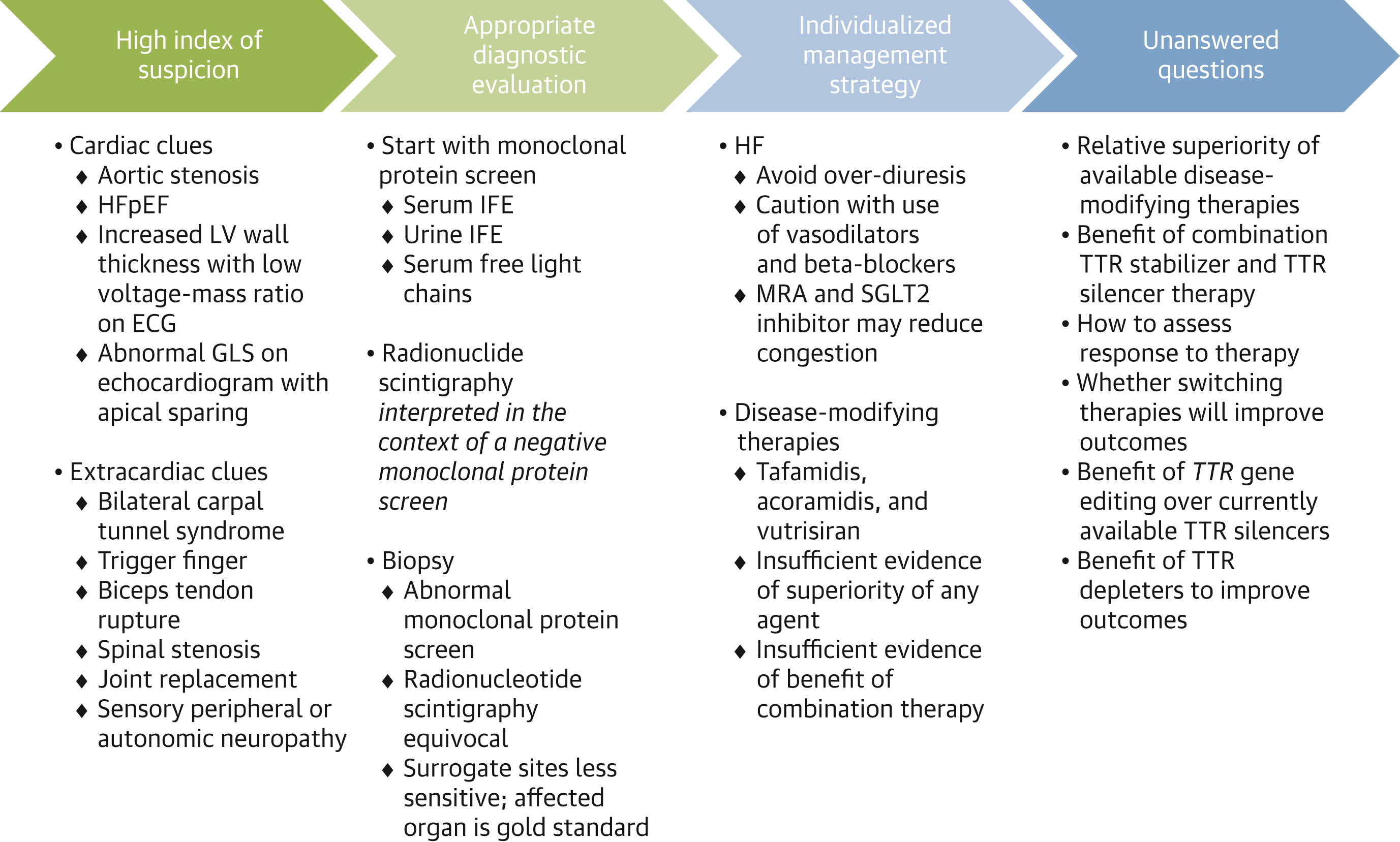
To help address these challenges and ensure care is taken "to avoid the most common diagnostic pitfalls," the CCG includes an algorithm for cardiac amyloidosis. According to the Writing Committee, chaired by Michelle M. Kittleson, MD, PhD, FACC, the "first and most critical step … is the exclusion of light chain amyloidosis."
Guidance on individual selection and choice of ATTR-CM disease-modifying therapies is another key component of the new document, taking into account new therapies over the last decade, including mineralocorticoid receptor antagonists and SGLT2 inhibitors, as well as specific disease-modifying therapies with transthyretin stabilizers (tafamidis and acoramidis) and the transthyretin silencer vutrisiran.
"The optimal time to start ATTR-CM disease-modifying therapy is at the earliest onset of symptomatic disease before significant end-organ dysfunction has ensued," the CCG states. A flow chart is provided to help clinicians determine when it is too early for disease-modifying therapy; when disease-modifying therapy is appropriate; and when it may be possibly too late.
Looking ahead, the CCG explores future therapies, such as transthyretin silencing with gene editing and transthyretin depleters with monoclonal antibodies, which hold promise but await further study. Additionally, it highlights several key unanswered questions tied to initial therapy; combination therapy and HF management; monitoring disease progression; prevention of disease; and cost-effectiveness.
"Clinicians now have multiple options to preserve the quality of life and improve the survival of individuals living with ATTR-CM," write the authors. "Although no studies presently demonstrate superiority of one agent over another, and although data are currently insufficient to recommend routine combination therapy and a change in therapy to mitigate disease progression, ongoing studies may help to clarify some of the unanswered questions to promote optimal care for individuals with ATTR-CM."
Clinical Topics: Heart Failure and Cardiomyopathies, Acute Heart Failure
Keywords: Mineralocorticoid Receptor Antagonists, Sodium-Glucose Transporter 2 Inhibitors, Prealbumin, Amyloidosis, Heart Failure, Cardiomyopathies
< Back to Listings