Nonobstructive HCM Treatment: Differential Effect of Bisoprolol vs. Verapamil
Bisoprolol but not verapamil reduced peak oxygen consumption (pVO2) in patients with nonobstructive hypertrophic cardiomyopathy (HCM), according to research published March 3 in JACC.
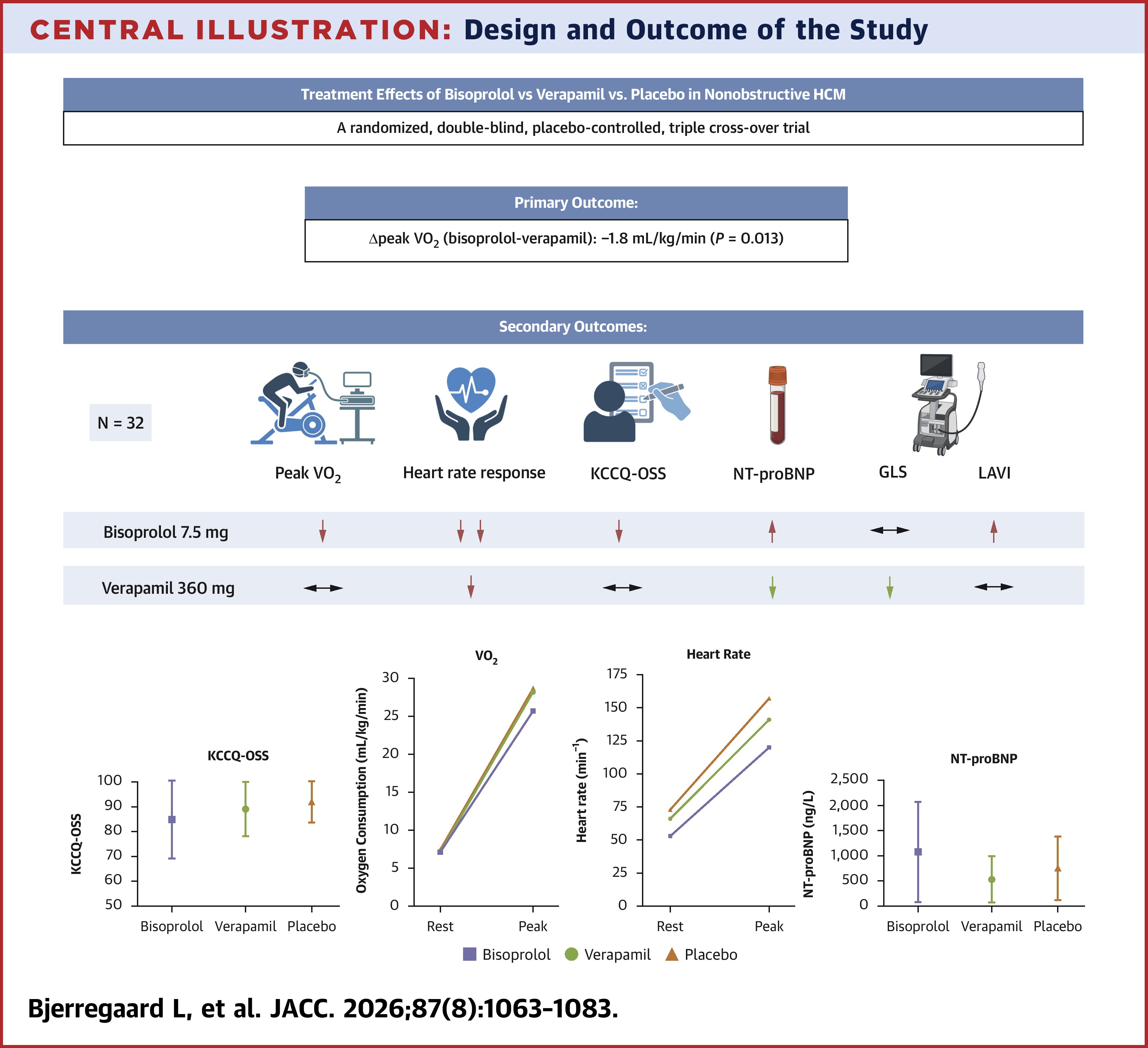
In this double-blinded, triple-crossover trial, researchers randomized 32 patients (mean age 54 years, 34% women) with nonobstructive HCM and at least one additional marker of disease severity (NYHA class ≥II, NT-proBNP >300 ng/L or nonsustained ventricular tachycardia (≥three consecutive ventricular beats >120 bpm within the two years preceding screening) to target doses of 7.5 mg bisoprolol, 360 mg verapamil or placebo. Each patient received all three treatments across a randomized sequence of three treatment periods.
For the primary endpoint of peak pVO2, results at two weeks of steady-state treatment showed it was 25.7 mL/kg/min with bisoprolol, 28.2 mL/kg/min with verapamil and 28.7 mL/kg/min with placebo. The adjusted mean differences were –1.8 mL/kg/min with bisoprolol vs. verapamil (p=0.013), –2.5 mL/kg/min with bisoprolol vs. placebo (p=0.002) and –0.7 mL/kg/min with verapamil vs. placebo (p=0.990).
Additionally, peak heart rate was lower with bisoprolol (–37 beats/min; p<0.001) and verapamil (–17 beats/min; p<0.001) vs. placebo. Neither drug changed oxygen consumption at anaerobic threshold or minute ventilation/CO2 production slope. Of note, verapamil but not bisoprolol improved global longitudinal strain.
Bisoprolol, vs. placebo, reduced the Kansas City Cardiomyopathy Questionnaire Overall Summary Score (KCCQ-OSS) by –6.6 points, increased NT-proBNP by 165 ng/L, increased left atrial volume index (LAVI) by 13.0 mL/m2 and increased tricuspid regurgitation (TR) pressure gradient by 4.3 mm Hg.
Verapamil, vs. placebo, did not change KCCQ-OSS (–2.3 points), LAVI (+5.2 mL/m2) or TR pressure gradients (+1.1 mm Hg) but did reduce NT-proBNP (–177 ng/L).
Study authors Louise Bjerregaard, MD, PhD, et al., note this is the first randomized head-to-head comparison of the beta-blocker bisoprolol and calcium channel blocker verapamil in a well-defined nonobstructive HCM cohort and that it provides novel insights into the effects of these conventional treatments on functional capacity, exercise response, myocardial function, structural changes, symptoms and biomarkers to inform clinical decision-making.
The different effect on pVO2 with bisoprolol and verapamil "may be explained by their distinct pharmacodynamic effects on the myocardium, resulting in different impacts on LV function," they write.
In an accompanying editorial comment, Martin S. Maron, MD, calls the decrease in exercise capacity with bisoprolol "significant, raising the critical question of whether the long-standing practice of administering [a beta-blocker] to nonobstructive HCM patients may potentially have had the unintended consequence of promoting unfavorable outcomes." Furthermore, he writes the data support a "necessary re-evaluation of [beta-blockers] for nonobstructive HCM, while also underscoring the priority of novel drug therapies to more effectively address the unmet treatment need for this patient subgroup."
Clinical Topics: Heart Failure and Cardiomyopathies, Acute Heart Failure
Keywords: Exercise Tolerance, Calcium Channel Blockers, Cardiomyopathy, Hypertrophic, Bisoprolol, Cardiomyopathies, Heart Failure, Verapamil
< Back to Listings