Is PCI Superior to Medical Therapy For CTO in Patients With CCS?
In patients with chronic coronary syndrome (CCS) with a single chronic total coronary occlusion (CTO) and no significant concomitant lesion, there was a greater improvement in quality of life (QoL) and symptom relief at 12 months, with no signal of excess harm, compared with optimal medical therapy (OMT), according to a post-hoc pooled analysis of the EUROCTO and DECISION-CTO trials published April 8 in JACC.
Gerald S. Werner, MD, FACC, and colleagues evaluated 518 patients with CCS and CTO (63 years old, 17% women, 35% with previous PCI) from the two open-label, multicenter trials that compared PCI and OMT. They used the Seattle Angina Questionnaire (SAQ) to assess clinical status at baseline and 12 months.
PCI was technically successful in 92.2% of patients. Crossover from OMT to PCI occurred in 6.7% of patients within the first year, while 3.7% of patients randomized to PCI did not undergo the procedure.
Results at 12 months showed significant improvement in patients with PCI over OMT in change in angina frequency (12.2 vs. 8.6; p=0.009), QoL (19.5 vs. 11.3; p<0.001) and SAQ summary score (13.8 vs. 8.5; p<0.001), respectively, in the intention-to-treat analysis.
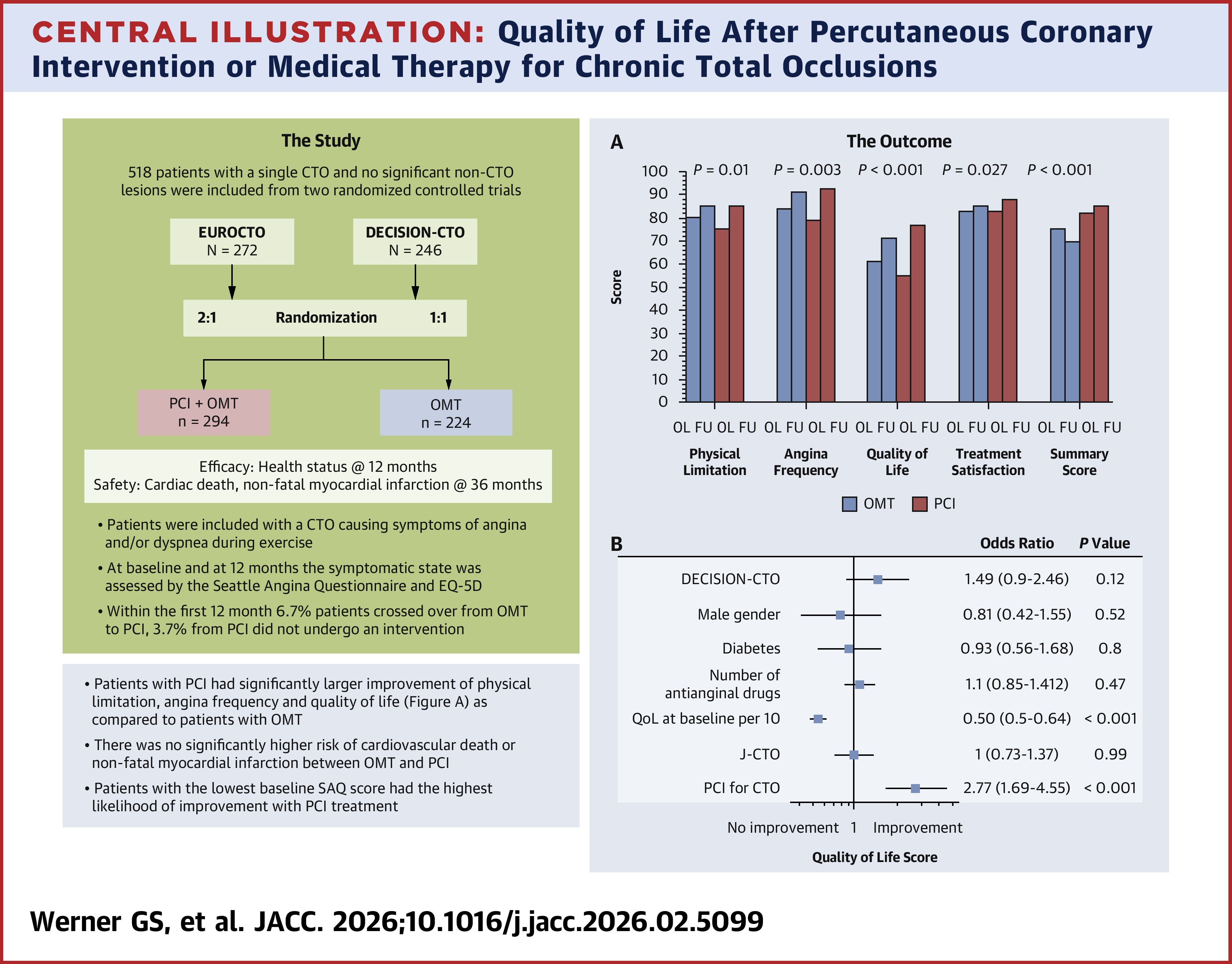
Clinically meaningful improvements were observed more often in the PCI group than with OMT for angina frequency (40.7% vs. 26.5%; p=0.002) and QoL (66.1% vs. 41.9%; p<0.001). Patients with the lowest baseline symptom score and QoL score were most likely to experience significant benefit with PCI. Demographic factors, diabetes status and lesion complexity did not independently predict improvement.
Over a mean follow-up of 3.1 years, the occurrence of clinical events was similar with PCI and OMT: cardiac death or nonfatal myocardial infarction (5.1% vs. 2.7%; p=0.17); the rates of stroke or hospitalization for bleeding were also similar.
Patients in the OMT group had higher rates of major cardiovascular and cerebrovascular events, largely driven by more ischemia-driven revascularization (18.8% vs. 10.6% with PCI; p=0.005).
"These results "may support the offer of revascularization for improvement of symptom and QoL in severely symptomatic CCS patients with a CTO rather than long-term antianginal medication," write the authors. However, they note that they "observed a wide individual variability in the symptomatic response, and that not all patients randomized to PCI would benefit." They add that further randomized trials are needed "to enhance our understanding of who would profit most from CTO PCI for symptom relief."
Clinical Topics: Invasive Cardiovascular Angiography and Intervention
Keywords: Percutaneous Coronary Intervention, Coronary Occlusion
< Back to Listings