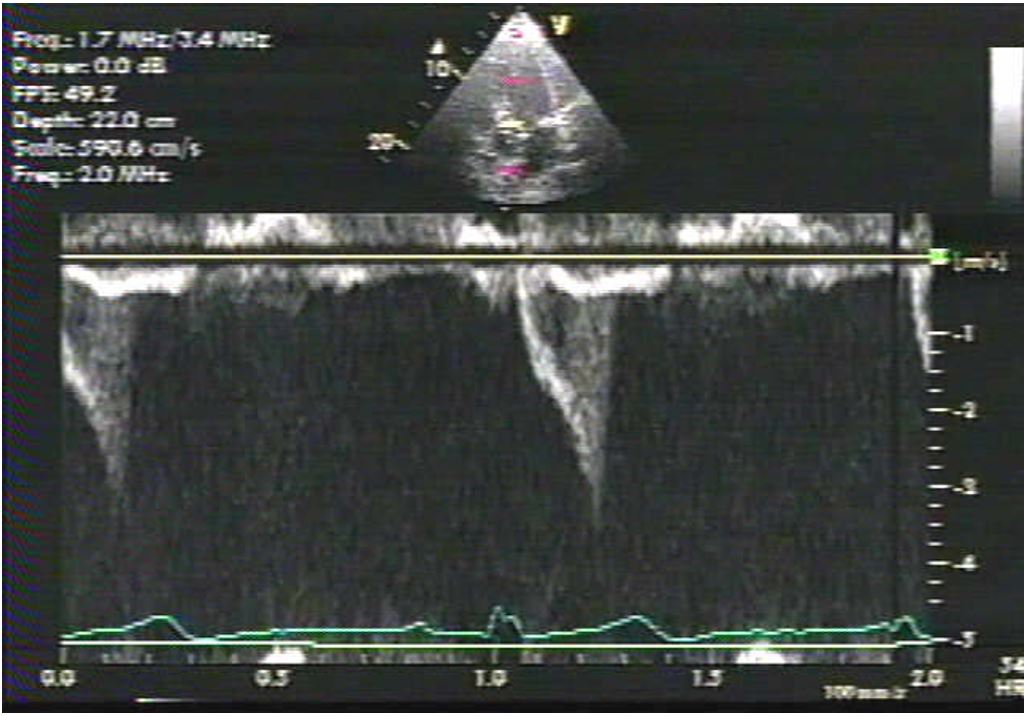
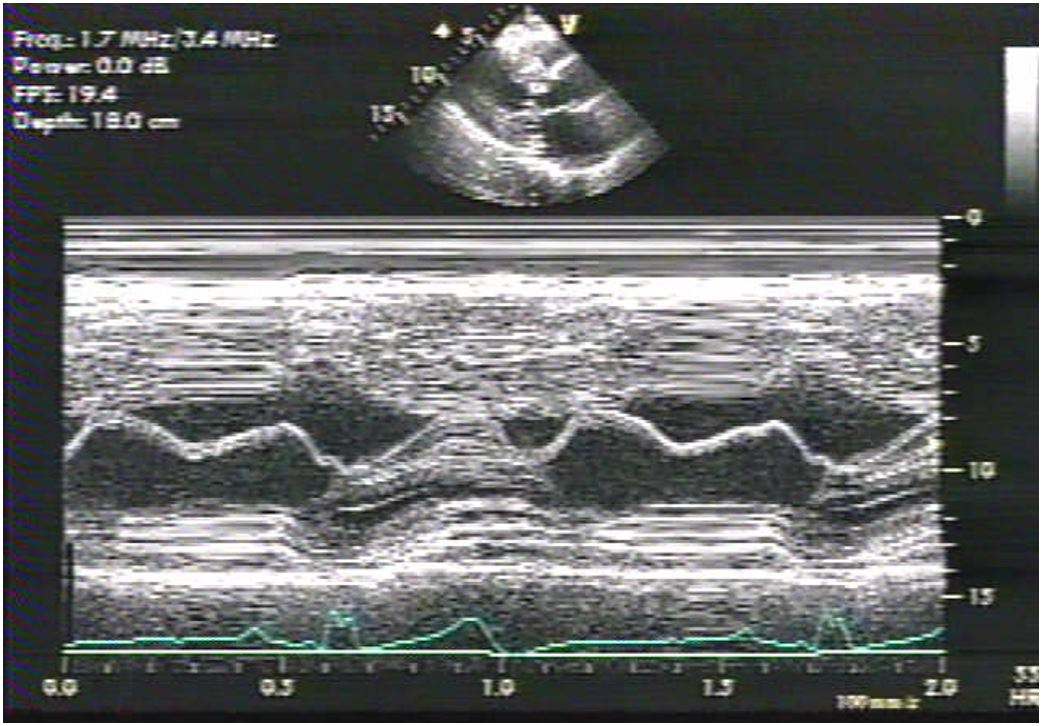
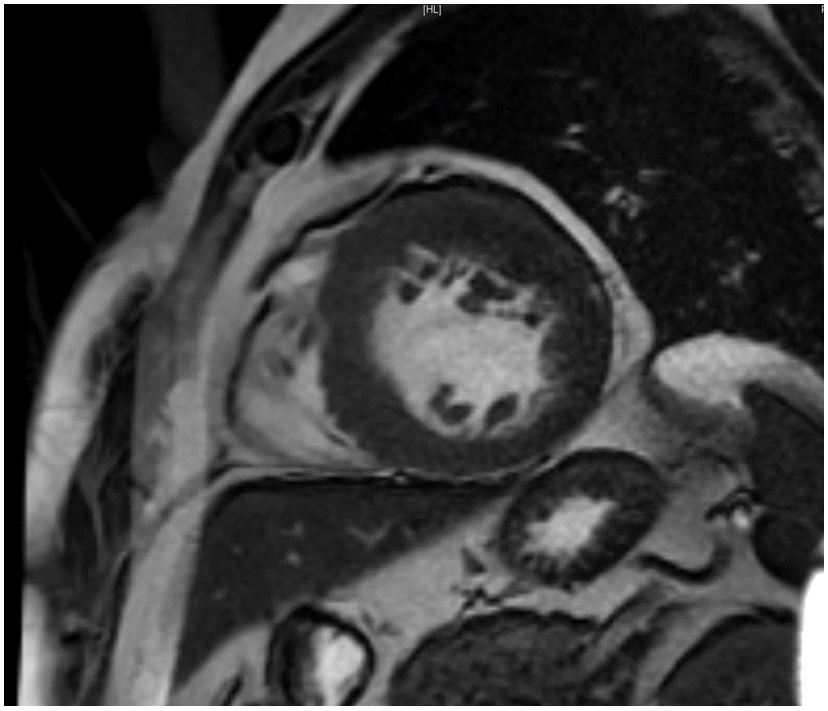
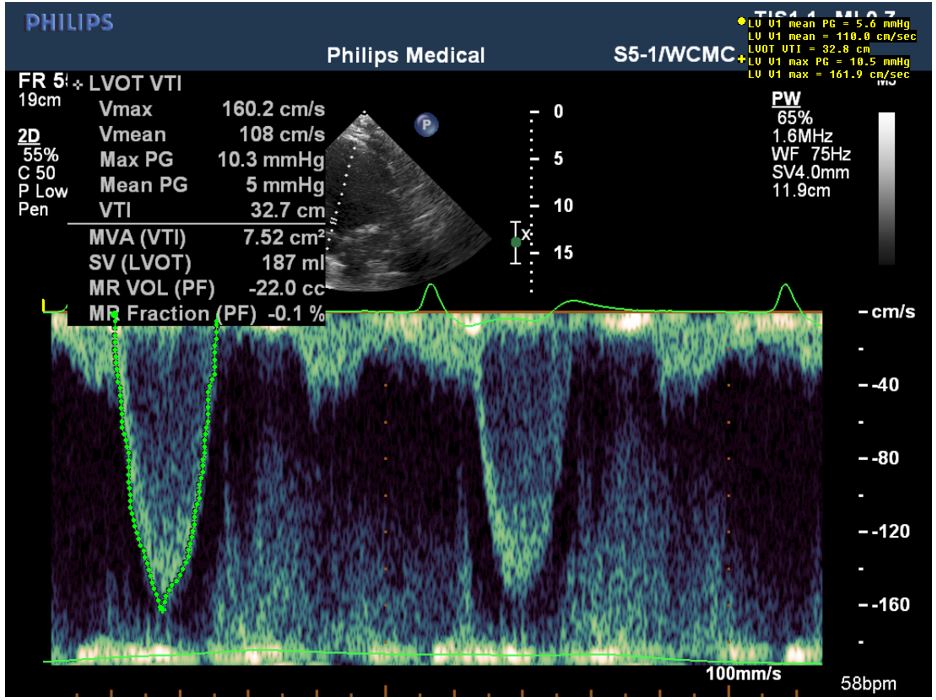
A 47-year-old man with hypertension, hyperlipidemia, and hypertrophic obstructive cardiomyopathy (HOCM) treated with atenolol and verapamil to maximally tolerated doses reports worsening dyspnea on exertion. He has a history of mild-to-moderate mitral regurgitation (MR) with a resting left ventricular outflow tract (LVOT) peak gradient of 49 mmHg (Figure 1), provokable to 60 mmHg with exercise. On exam, his blood pressure is 125/80 mmHg with a resting heart rate of 53 bpm. He has a III/VI harsh mid-systolic murmur at the left lower sternal border and a II/VI mid-systolic murmur at the apex. Disopyramide therapy is aborted due to excessive QT prolongation. An echocardiogram demonstrates a septal thickness of 2.0 cm, a normal ejection fraction of 66%, and systolic anterior motion of the mitral leaflets with 4+ severe MR and 1+ mild aortic regurgitation (Figure 2, Videos 1-3). Cardiac magnetic resonance imaging confirms these findings along with severe left atrial enlargement and anterior displacement of the anterior papillary muscle (Figure 3, Video 4).
Figure 1
Figure 2
Video 1
Video 2
Video 3
Figure 3
Video 4
What should you recommend to this patient to best treat his MR?
Show Answer
The correct answer is: D. Surgical septal myectomy with intraoperative reassessement of MR
This patient has HOCM with LVOT obstruction with a provokable gradient >50 mmHg and is symptomatic despite maximally tolerated medical therapy; therefore, septal reduction therapy is advised.
MR is common in HOCM due to distortion of the mitral valve apparatus from systolic anterior motion secondary to LVOT obstruction.1 In most cases, intrinsic mitral valve disease is not present, and MR is most often relieved with surgical septal myectomy alone without the need for additional mitral valve intervention. As demonstrated in the review by Hong et al.,2 of 1,905 septal myectomies performed at the Mayo Clinic from 1993 to 2014, 96.1% were treated without mitral valve intervention with a reduction in the prevalence of severe MR from 54.3 to 1.7% on early post-operative echocardiography. Only 75 patients required concomitant mitral valve repair or replacement. This study was limited, however, by a lack of data regarding morphometric measurements of the mitral valve such as leaflet length, a lack of uniform availability of cardiac magnetic resonance imaging data, and a lack of long-term outcomes with echocardiographic assessment of MR.
Per the 2011 American College of Cardiology and American Heart Association Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy,1 this patient has no significant risk factors that would make surgical myectomy high risk or contraindicated, and so surgical myectomy rather than alcohol septal ablation should be recommended (Class IIa recommendation). If the patient expressed a preference to avoid surgery after a balanced and thorough discussion, then alcohol septal ablation could be considered as an alternative (Class IIb recommendation.)
Although the mitral leaflet (particularly the anterior) can be elongated in patients with hypertrophic cardiomyopathy, there would be no need to attempt repair or plication of the mitral valve to treat the MR in this patient unless the MR did not improve following septal myectomy. Sherrid et al.3 noted that anterior displacement of the anterolateral papillary muscle is a common pathogenic abnormality in HOCM. In such cases, an extended myectomy that involves release of the anterolateral papillary muscle may be advisable because this may allow a more normal parallel orientation of the mitral annulus and aortic valve. Examination of the muscular connections between the papillary muscle head and the left ventricle free wall should be performed during myectomy to determine what additional measures may be required to maximize the relief of systolic anterior motion and LVOT obstruction. Additional anomalies could include insertion of the anterolateral papillary muscle directly into the anterior leaflet, fibrotic or retracted secondary chordae, and elongation of the posterior leaflet.
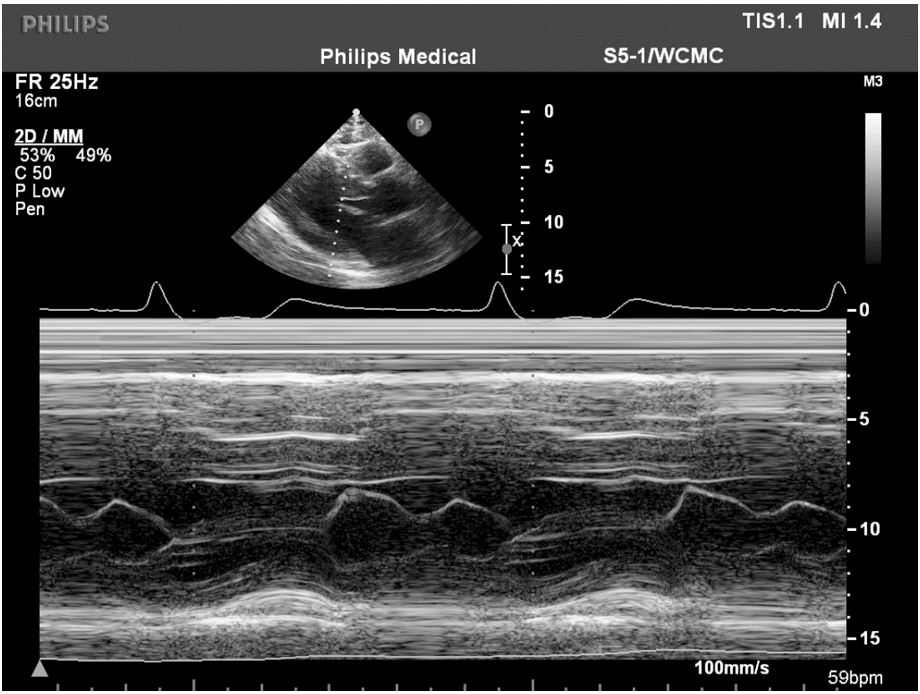
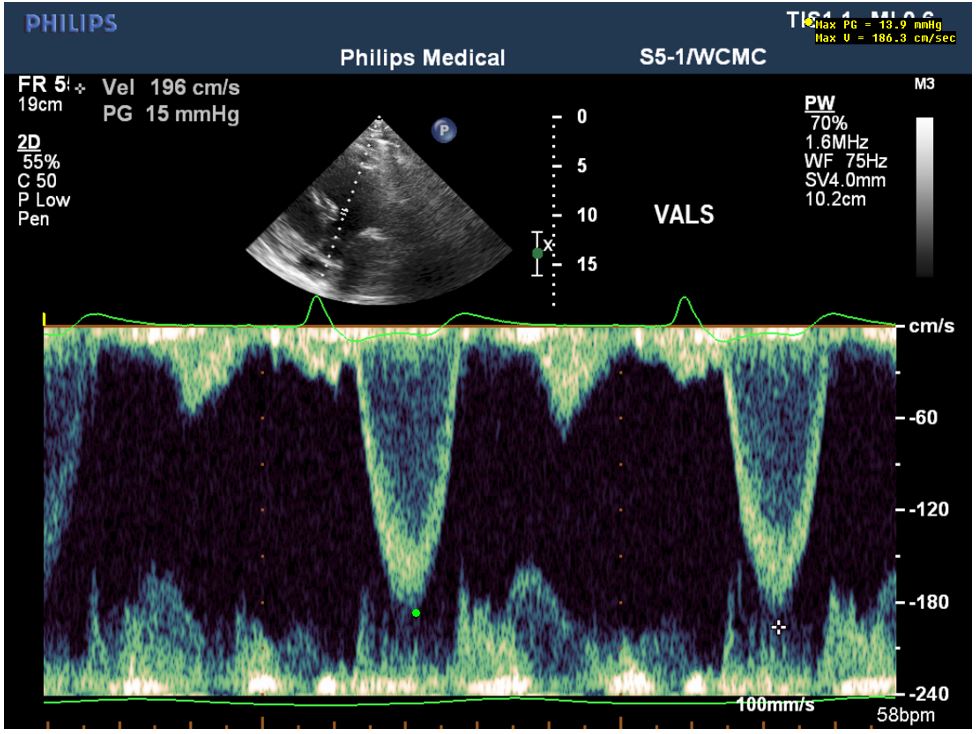
This patient agreed to surgical septal myectomy, which was performed with wide and deep margins with relief of LVOT obstruction without the need for additional surgical interventions. He had trace MR following surgery with no resting gradient and a provokable gradient of only 14 mmHg with Valsalva maneuver (Videos 5-6, Figures 4-6.)
Video 5
Video 6
Figure 4
Figure 5
Figure 6
References
Gersh BJ, Margon BJ, Bonow RO, et al. 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collaboration with the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2011;58:e212-60.
Hong JH, Schaff HV, Nishimura RA, et al. Mitral Regurgitation in Patients With Hypertrophic Obstructive Cardiomyopathy: Implications for Concomitant Valve Procedures. J Am Coll Cardiol 2016;68:1497-504.
Sherrid MV, Balaram S, Kim B, Axel L, Swistel DG. The Mitral Valve in Obstructive Hypertrophic Cardiomyopathy: A Test in Context. J Am Coll Cardiol 2016;67:1846-58.