A 74-year-old male patient with a history of chronic kidney disease stage III and paroxysmal atrial fibrillation was referred to cardiology with profound shortness of breath with exertion. He was previously quite active and hiked frequently in the deserts of Arizona. Over the last 6 months, he noted inability to complete his usual hiking routes and labored breathing with simple activities such as showering and household chores. He had normal vital signs, and his exam was remarkable for a well-built male in no acute distress. His lungs were clear to auscultation. His heart rate was regular with a split S2 with inspiration, no S3/S4, and no murmurs, rubs, clicks, gallops, or edema. His neck veins were elevated to 9 cm H20, and the hepatojugular reflex was negative. Pulmonary function testing was unremarkable for his age, and an electrocardiogram demonstrated sinus rhythm with first degree atrioventricular block and right axis deviation.
He underwent stress echocardiogram. At rest, his left ventricular ejection fraction was 55%, which increased to 70% at peak exertion. Echocardiographic evaluation of the right heart noted resting right ventricular systolic pressure of 50 mmHg, tricuspid annular plane systolic excursion of 15 mm, and fractional area change of 35%. Stress images captured a peak tricuspid regurgitation jet of 3.75 m/s. No wall motion abnormalities or septal bowing were seen. He was referred for right heart catheterization with invasive cardiopulmonary exercise testing. Pulmonary artery and right atrial wave forms and hemodynamic data are shown in Figure 1 and Table 1.
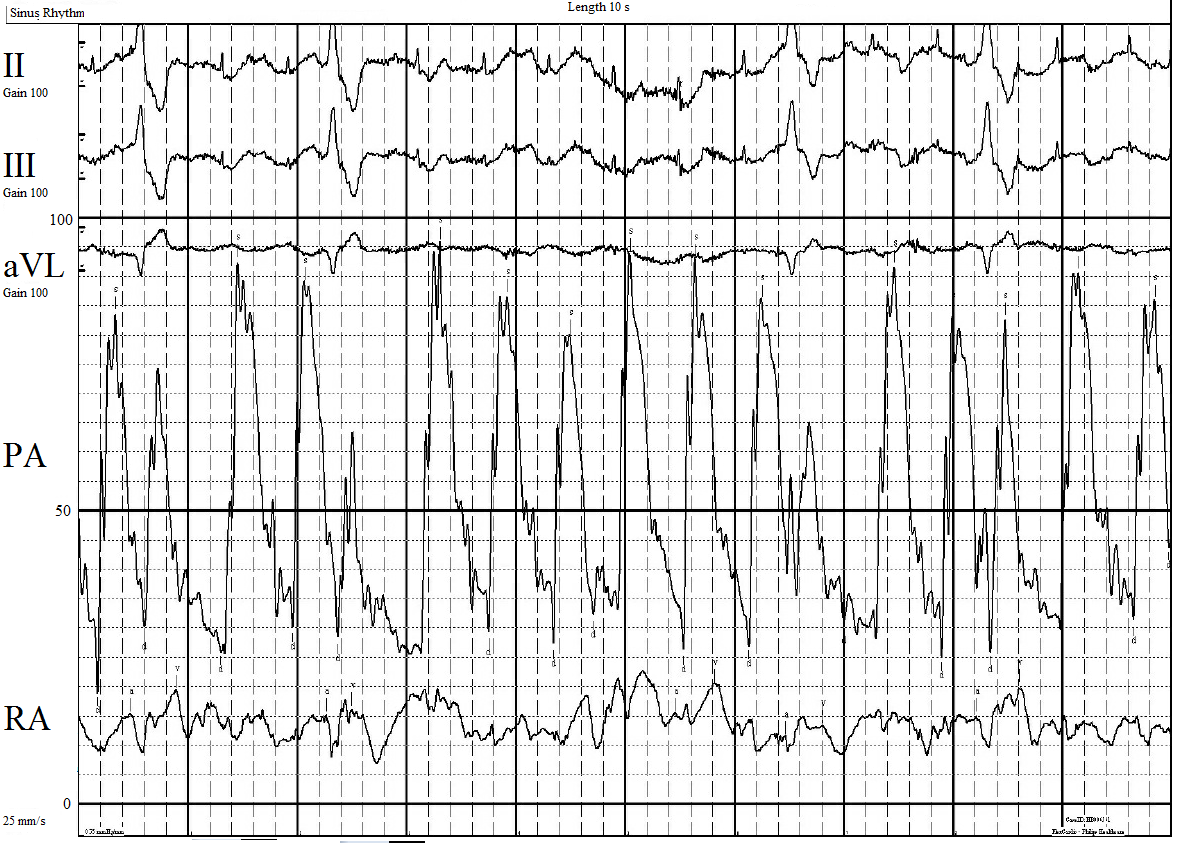
Figure 1: Telemetry, Pulmonary Artery, and Right Atrial Wave Forms at 60 Watts Workload
Figure 1
Scale set to 100 mmHg.
Scale set to 100 mmHg.
Table 1: Right Heart Catherization Data at Rest and at Peak Exertion
Values reported as systolic/diastolic and (mean pressure).
Given the patient's hemodynamic data, which of the following medications is indicated for therapy?
Show Answer
The correct answer is: E. No therapy is currently indicated
Pulmonary arterial hypertension is defined as a resting pulmonary artery pressure greater than 25 mmHg with pulmonary vascular resistance (PVR) in excess of 3 Wood units and a pulmonary capillary occlusion pressure (PCOP) less than 15 mmHg.1 The patient does not meet criteria for pulmonary hypertension at rest; however, his pulmonary arterial pressures increase dramatically with exercise. At peak exertion he meets criteria for exercise pulmonary hypertension. Patients with exercise pulmonary hypertension have normal pulmonary artery pressures at rest, but with exertion the mean pulmonary arterial pressure (mPAP) increases to >30 mmHg with a normal PCOP.2 Currently, there is no consensus as to treatment for exercise pulmonary hypertension.
When interpreting hemodynamic data, changes in pulmonary pressure must be viewed in the context of flow through the pulmonary circulation. The mPAP is a function of the cardiac output (Q), PVR, and the left atrial pressure, which in practice is measured by the PCOP:
mPAP = Q x PVR + PCOP
In the healthy subject, mPAP will increase with exercise as increases in flow (Q) occur through the pulmonary vasculature bed and into the left atrium. The alteration in pressure is balanced by a drop in PVR from recruitment of the normally compliant pulmonary vasculature:3,4
↑mPAP = ↑Q x ↓PVR + ↑PCOP
With development of occult pulmonary vascular disease, the compliance of the pulmonary vasculature is lost, and PVR begins to increase. Symptoms of dyspnea and exercise intolerance have been correlated with mPAP in excess of 30 mmHg with exertion. Tolle et al. retrospectively evaluated 406 patients with exertional dyspnea and discovered that those patients who meet the criteria for exercise pulmonary hypertension had lower maximal oxygen uptake, right ventricular ejection fraction, and higher PVR than controls; yet these hemodynamic markers were not as adverse as those in patients who have elevated pulmonary arterial pressures at rest.2 The European Respiratory Society currently advises that exercise pulmonary hypertension requires follow-up, especially if risk factors for pulmonary hypertension are present.3 Furthermore, exercise pulmonary hypertension has been associated with systemic sclerosis, left heart disease, chronic lung disease, and chronic thromboembolism.5
It is yet unknown if patients with dyspnea and exercise pulmonary hypertension benefit from pulmonary vasodilator therapy. The endothelin receptor antagonists have been used for treatment of exercise pulmonary hypertension in small pilot studies. Bosentan (answer A) has been noted to improve hemodynamics in a study of 10 patients with connective tissue disease and exercise pulmonary hypertension,6 but further studies are needed before this drug is accepted for widespread use in exercise pulmonary hypertension. Ambrisentan has also been studied in another small pilot study of 11 patients and found to improve exercise pulmonary arterial pressures, PVR, and clinically meaningful 6-minute walk distance.7 Sildenafil (answer B), prostacyclin therapy (answer C), and the guanylate cyclase stimulator riociguat (answer D) have not yet been studied in this population.
References
Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 2016;37:67-119.
Tolle JJ, Waxman AB, Van Horn TL, Pappagianopoulos PP, Systrom DM. Exercise-induced pulmonary arterial hypertension. Circulation 2008;118:2183-9.
Kovacs G, Herve P, Barbera JA, et al. An official European Respiratory Society statement: pulmonary haemodynamics during exercise. Eur Respir J 2017;50:1700578.
Naeije R, Vanderpool R, Dhakal BP. Exercise-induced pulmonary hypertension: physiological basis and methodological concerns. Am J Respir Crit Care Med 2013;187:576-83.
Naeije R, Saggar R, Badesch D, et al. Exercise-Induced Pulmonary Hypertension: Translating Pathophysiological Concepts Into Clinical Practice. Chest 2018;154:10-5.
Kovacs G, Maier R, Aberer E, et al. Pulmonary arterial hypertension therapy may be safe and effective in patients with systemic sclerosis and borderline pulmonary artery pressure. Arthritis Rheum 2012;64:1257-62.
Saggar R, Khanna D, Shapiro S, et al. Brief report: effect of ambrisentan treatment on exercise-induced pulmonary hypertension in systemic sclerosis: a prospective single-center, open-label pilot study. Arthritis Rheum 2012;64:4072-7.