The patient is a 65-year-old woman with a medical history of hypertension, supraventricular tachycardia, prior tobacco use, right renal cell carcinoma (status post partial nephrectomy), metastatic right breast invasive ductal carcinoma (status post segmental mastectomy), complete axillary dissection, and breast reconstruction who was hospitalized for bilateral breast cellulitis requiring breast implant exchange and developed post-operative asymptomatic paroxysmal supraventricular tachycardia with heart rate up to 161 bpm. At presentation, her physical exam was remarkable for bilateral surgical wounds in the breast area. An electrocardiogram showed anterolateral and inferior T-wave inversions. Troponin I was elevated at 0.79 ng/mL, and creatine kinase-muscle/brain was elevated at 7 ng/mL. An echocardiogram was technically difficult, and left ventricular (LV) function assessment was limited. A nuclear stress test was obtained (Figures 1-2).
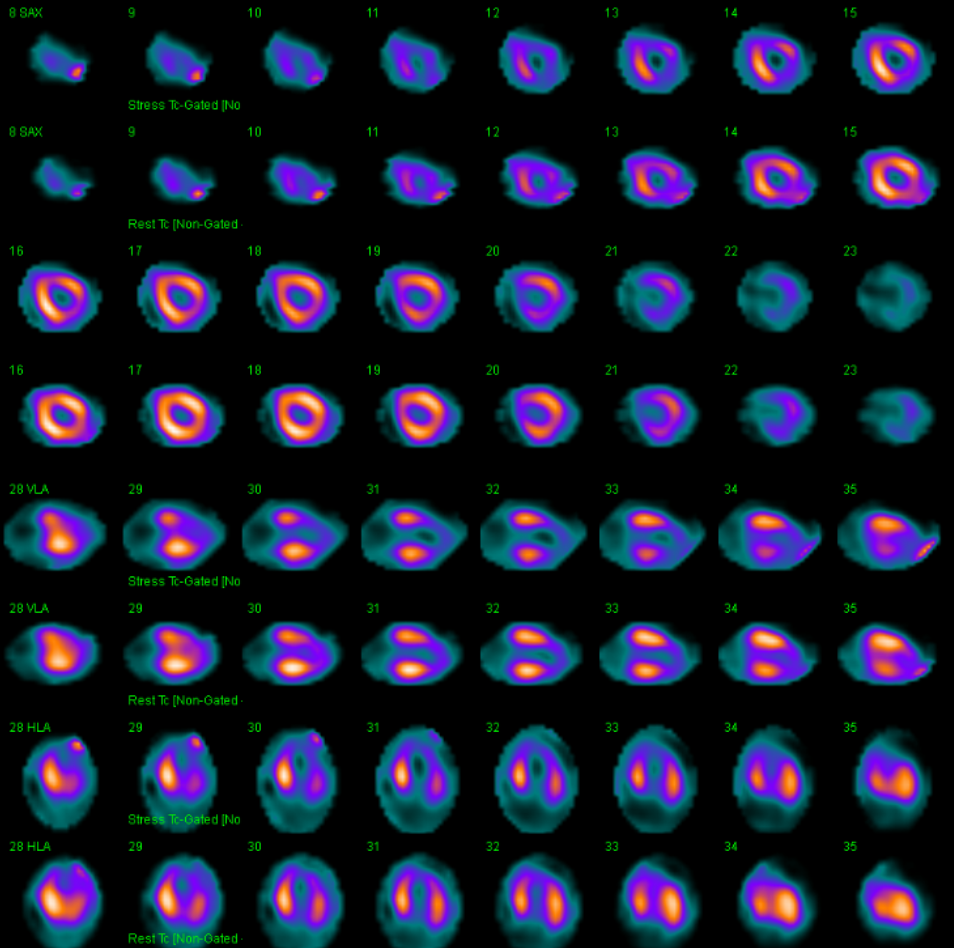
Figure 1
Figure 1
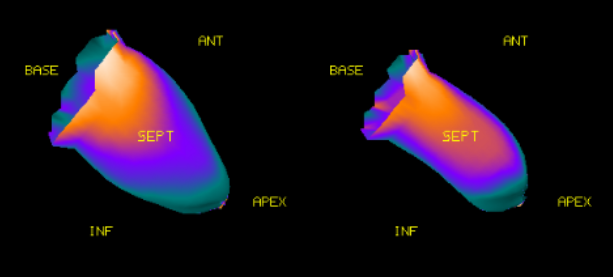
Figure 2
Figure 2
Regarding the single-photon emission computed tomography (SPECT) images, which of the following is the best interpretation and next step in management?
Show Answer
The correct answer is: B. The patient has areas of ischemia; proceed with coronary angiography.
The SPECT images demonstrate a large area from the mid ventricle to the apex with significant myocardial thinning and a perfusion defect at rest that worsens moderately during stress. The basal segments are spared. This pattern of reversibility is suspicious for a dominant left anterior descending artery that wraps around the apex; however, the basal sparing is atypical. The LV function was calculated at 51%. A diagnosis of Takotsubo cardiomyopathy was suggested; however, exclusion of obstructive coronary disease is needed. The patient underwent coronary angiogram, which showed 50% stenosis of the left anterior descending artery and severe hypokinesis of the apical wall of the LV with hyperdynamic basal segments, typical for Takotsubo cardiomyopathy.
Takotsubo cardiomyopathy is characterized by severe LV dysfunction that recovers spontaneously within days or weeks. It is thought to be mediated by acute catecholaminergic myocardial stunning, with an epinephrine-induced beta-2 adrenergic receptor-mediated regional akinesia of the LV apex and mid-ventricle, and LV outflow tract obstruction caused by norepinephrine-induced hyperkinesia of the basal region.1-3 The revised Mayo clinic criteria for Takotsubo cardiomyopathy diagnosis include 1) the presence of a transient abnormality in LV wall motion beyond a single epicardial coronary artery perfusion territory, 2) the absence of obstructive coronary artery disease or angiographic evidence of acute plaque rupture, 3) the presence of new electrocardiographic abnormalities or elevation in cardiac troponin levels, and 4) the absence of pheochromocytoma and myocarditis.3,4 The long-term prognosis of patients with Takotsubo cardiomyopathy is comparable to that of patients with acute coronary syndrome.5
Radionuclide imaging techniques have been successfully employed in the differential diagnosis of Takotsubo cardiomyopathy from acute coronary syndrome. SPECT using 99mTc can detect reversible perfusion defects that extend in an atypical distribution for coronary artery disease, like in our patient. Other radiotracers such as iodine-123 metaiodobenzylguanidine (mIBG), a gamma-emitting norepinephrine analogue, have been used to visualize cardiac sympathetic nerve activity, and reduced uptake has been shown in dysfunctional myocardial segments, consistent with a regional disturbance of sympathetic neuronal activity. These abnormalities can persist for months; therefore, radionuclide imaging may have a role in cases without a diagnosis or when the presentation is remote from an acute episode.6,7
Cardiac positron-emission tomography using [18F]2-fluoro-deoxy-glucose demonstrated decreased radionuclide uptake in patients with this cardiomyopathy despite a relatively normal perfusion. This association is commonly known as inverse metabolic-perfusion mismatch and represents a transient metabolic disorder at the cellular level, demonstrated by evidence of tissue's impaired metabolism in the dysfunctioning LV with preserved myocardial blood flow at rest.8
Sardu C, Sacra C, Mauro C, Siniscalchi M, Marfella R, Rizzo MR. 123I-MIBG Scintigraphy in the Subacute State of Takotsubo Cardiomyopathy. JACC Cardiovasc Imaging 2017;10:93-4.
Medina de Chazal H, Del Buono MG, Keyser-Marcus L, et al. Stress Cardiomyopathy Diagnosis and Treatment: JACC State-of-the-Art Review. J Am Coll Cardiol 2018;72:1955-71.
Templin C, Ghadri JR, Diekmann J, et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N Engl J Med 2015;373:929-38.
Ghadri JR, Kato K, Cammann VL, et al. Long-Term Prognosis of Patients With Takotsubo Syndrome. J Am Coll Cardiol 2018;72:874-82.
Lyon AR, Bossone E, Schneider B, et al. Current state of knowledge on Takotsubo syndrome: a Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2016;18:8-27.
Citro R, Pontone G, Pace L, et al. Contemporary Imaging in Takotsubo Syndrome. Heart Fail Clin 2016;12:559-75.
Testa M, Feola M. Usefulness of myocardial positron emission tomography/nuclear imaging in Takotsubo cardiomyopathy. World J Radiol 2014;6:502-6.