ACS in the Setting of Coronary Ectasia: A Challenging Case
Jun 07, 2019
|
Font Size
A
A
A
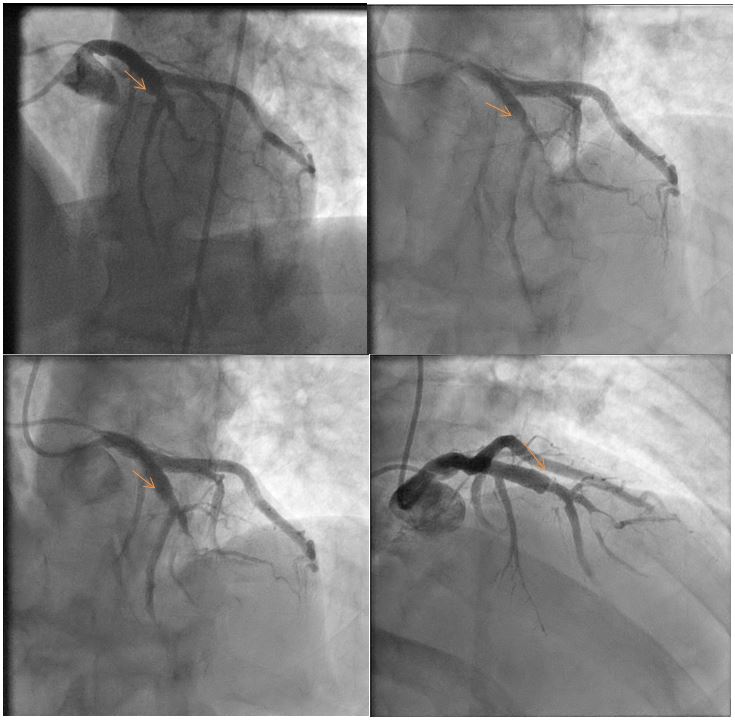
A 59-year-old male nonsmoker with medical history of hypertension, strong family history of premature coronary artery disease, and an incidental pancreatic mass was scheduled for biopsy in a week. The patient presented to the emergency department with substernal chest pain. The electrocardiogram was normal. Laboratory evaluation was significant for an elevated troponin I (27 ng/ml). A transthoracic echocardiogram demonstrated normal left ventricular systolic function without wall motion abnormalities. The patient underwent urgent cardiac catheterization for non-ST-segment elevation myocardial infarction (NSTEMI). Findings were a large caliber dominant right coronary artery with mild proximal disease and ectasia with slow flow and proximal left anterior descending (LAD) ectasia with evidence of a ruptured plaque in the mid-segment (just before the takeoff of a bifurcating diagonal branch) with Thrombolysis in Myocardial Infarction 2 flow in the distal LAD. Intravascular ultrasound of the LAD demonstrated a very large caliber vessel with a non-occlusive ruptured plaque in the mid-vessel. Instantaneous wave-free ratio of the mid-LAD culprit lesion was 0.97, consistent with non-significant residual stenosis.
Which of the following is true regarding this patient's condition?
Show Answer
The correct answer is: B. The best approach is to defer percutaneous coronary intervention (PCI) and treat medically with antiplatelet therapy and high-intensity statin.
The patient presented with NSTEMI related to plaque rupture within the ectatic segment of the LAD. Although an NSTEMI is often treated with PCI, this patient had adequate distal flow, instantaneous wave-free ratio testing was negative for significant functional stenosis, and intravascular ultrasound showed mild residual disease. Furthermore, the patient required a pancreatic biopsy, and mandatory dual antiplatelet therapy after PCI would lead to an increased risk of this procedure. In adult patients, coronary ectasia is most often caused by atherosclerosis. In children and young adults, vasculitis (e.g., Kawasaki disease) is far more common. Interestingly, patients with diabetes mellitus have low incidence of coronary ectasia. Based on the significant flow disturbances within the ectatic segments, chronic anticoagulation with warfarin has been suggested. However, this approach has not been tested prospectively; therefore, the decision to treat with oral anticoagulation should be individualized.
Figure 1: Different Views Showing the Ectatic Proximal LAD and the Slow Flow After the Stenosis
Aboeata AS, Sontineni SP, Alla VM, Esterbrooks DJ. Coronary artery ectasia: current concepts and interventions. Front Biosci (Elite Ed) 2012;4:300-10.
Fineschi M, Gori T, Sinicropi G, Bravi A. Polytetrafluoroethylene (PTFE) covered stents for the treatment of coronary artery aneurysms. Heart 2004;90:490.
Demopoulos VP, Olympios CD, Fakiolas CN, et al. The natural history of aneurysmal coronary artery disease. Heart 1997;78:136-41.
Friedman KG, Gauvreau K, Hamaoka-Okamoto A, et al. Coronary Artery Aneurysms in Kawasaki Disease: Risk Factors for Progressive Disease and Adverse Cardiac Events in the US Population. J Am Heart Assoc 2016;5:e003289.
Pijls NH, van Schaardenburgh P, Manoharan G, et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER Study. J Am Coll Cardiol 2007;49:2105-11.
Doi T, Kataoka Y, Noguchi T, et al. Coronary Artery Ectasia Predicts Future Cardiac Events in Patients With Acute Myocardial Infarction. Arterioscler Thromb Vasc Biol 2017;37:2350-5.