A 53-year-old woman with hypertension, hyperlipidemia, anxiety disorder, and a remote surgical history of bilateral salpingo-oophorectomy presented with chest pain. She was in her usual state of good health until the day of admission, when she developed chest discomfort while moving furniture in her apartment. She reported that her symptoms were sub-sternal, left-sided, and 7/10 in severity, with chest pain radiating to her left arm and jaw. She also reported mild dyspnea and an episode of nausea. The symptoms lasted 30 minutes and gradually resolved with rest. She activated emergency medical services and was brought to the hospital by ambulance for further evaluation.
In the emergency department, the patient was free of chest pain. Physical examination was notable for an overweight woman in no acute distress. Body temperature was 98.6 F˚, pulse was 102 bpm, blood pressure was 153/78, respiratory rate was 14 breaths per minute, and oxygen saturation was 100% on room air. Cardiovascular examination revealed a normal S1 and S2 without murmurs, rubs, or gallops. There was no jugular venous distention or lower extremity edema. Pulses were 2+ and symmetric.
The initial troponin-I was elevated to 3.13 ng/mL. Complete blood count revealed a mild leukocytosis of 11.6 k/uL, hemoglobin of 13.0 g/dL, and platelets of 192 K/uL. A comprehensive metabolic panel was notable for normal renal function with a blood urea nitrogen of 11 and a creatinine of 0.6. Total cholesterol was 211 mg/dL (high-density lipoprotein cholesterol of 41 mg/dL, low-density lipoprotein cholesterol of 137 mg/dL, and triglycerides of 163 mg/dL).
Electrocardiography in the emergency department revealed normal sinus rhythm with no significant ST-segment or T-wave changes. No cardiopulmonary pathology was evident on a chest radiograph. Echocardiography was notable for a left ventricular (LV) ejection fraction of 55%, with hypokinesis of the basal interventricular septum. There was no significant valvular disease.
Based on her clinical presentation, the patient was diagnosed with myocardial infarction (MI), and 325 mg of aspirin, 300 mg of clopidogrel, and a high-intensity statin were administered. She was referred for invasive coronary angiography.
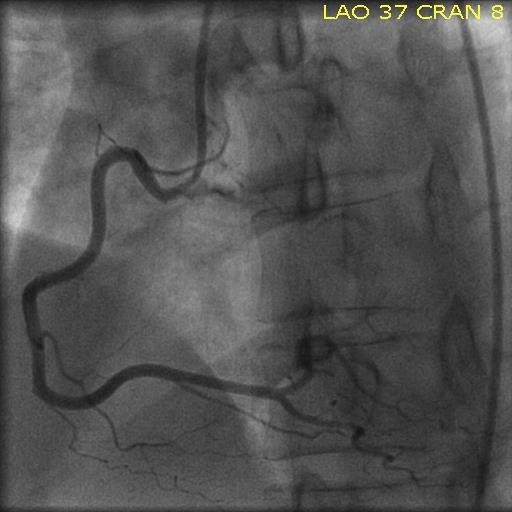
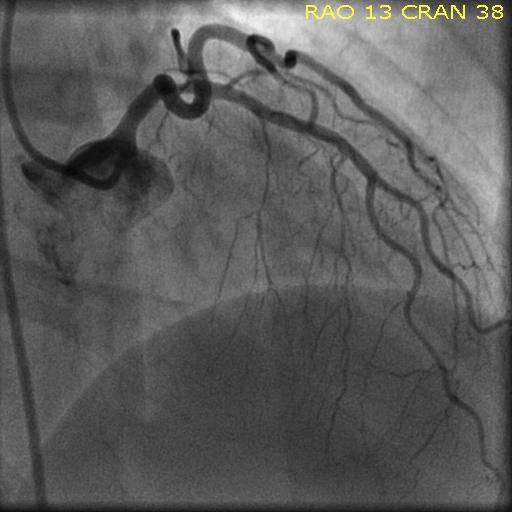
Invasive coronary angiography revealed angiographically normal right coronary (Figure 1) and left main and circumflex arteries (Figure 2). There was mild coronary artery disease in the proximal left anterior descending artery (LAD). The LV end diastolic pressure was <5 mmHg. A diagnosis of MI with nonobstructive coronary arteries (MINOCA) was established.
Figure 1: Coronary Angiography of the Right Coronary Artery System in the Left Anterior Oblique View With Slight Cranial Angulation
Figure 1
Figure 2: Coronary Angiography of the Left Coronary Artery System in the Right Anterior Oblique View With Cranial Angulation
Figure 2
Which of the following diagnostic steps is the most appropriate to establish the mechanism of MINOCA?
Show Answer
The correct answer is: E. Choices B & D
MINOCA occurs in 6% of MI and is 3 times more common among women than men.1-3 An international standardized definition for MINOCA was recently established by the European Society of Cardiology and American Heart Association.4,5 MINOCA requires a diagnosis of MI that
meets the universal MI definition,1
has <50% angiographic stenosis in all major epicardial vessels (including normal coronary arteries or mild-to-moderate atherosclerosis), and
does not have a clinically overt alternate explanations for the MI presentation, such as heart failure, sepsis, or pulmonary embolism.4,5
Although MINOCA is associated with a more favorable prognosis than MI with obstructive coronary artery disease, MINOCA can be fatal; 17% of decedents with pathologic evidence of MI at autopsy have no obstructive coronary artery disease.6 Early in-hospital mortality after MINOCA presentation is 1.1%, and MINOCA patients who survive to hospital discharge have a 4.7% risk of mortality at 1 year.2,7 In contrast to MI with coronary artery disease, which is typically mediated by unstable atherosclerotic plaque, MINOCA can have varied underlying causes.4 Mechanisms of MINOCA may include plaque erosion, plaque rupture, in-situ non-occlusive thrombosis, thrombotic occlusion with thrombolysis or distal embolization, flush occlusion of a branch vessel, spontaneous coronary artery dissection, epicardial coronary spasm, and coronary microvascular dysfunction.3,8
The diagnosis of plaque disruption can be definitively established with high-resolution intracoronary imaging with IVUS or OCT (answer B). Intracoronary imaging can also establish a diagnosis of spontaneous coronary artery dissection when it is not angiographically apparent. The American Heart Association Scientific Statement on MINOCA recommends that, "if available, OCT or IVUS imaging be performed in patients with MINOCA and evidence of nonobstructive atherosclerosis on an angiogram."9 Intravascular imaging with OCT may be preferred to IVUS given the higher imaging resolution.9
CMRI can confirm the diagnosis of MI and exclude related syndromes that may mimic MINOCA (answer D). Patients with myocarditis and takotsubo syndrome also typically present with chest pain, electrocardiographic changes, abnormal cardiac biomarkers, and new wall motion abnormalities that may be suggestive of MI. Coronary angiography in these cases typically reveals nonobstructive coronary artery disease. Takotsubo syndrome is characterized by transient LV dysfunction with a regional wall motion abnormality that usually extends beyond the vascular distribution of a single coronary artery. Takotsubo syndrome typically presents after a physical or emotional trigger and is more common in women than men. Myocarditis is more common in younger individuals, those without coronary artery disease risk factors, and in patients with fevers or a recent viral illness. A diagnosis of myocarditis should be suspected when there is imaging evidence of myocardial edema on T2-weighted CMRI images, characteristic gadolinium-enhanced T1-weighted images with early enhancement, and late gadolinium enhancement of the sub-epicardium or mid-wall in a non-coronary distribution. When MI has occurred, sub-endocardial or transmural late gadolinium enhancement by CMRI may be seen in a coronary distribution, although the absence of MI by CMRI does not exclude a diagnosis of MINOCA. CMRI also provides reliable measures of ventricular function, chamber size, myocardial thickness, and wall motion abnormalities. Based on these advantages, CMRI "is recommended as a key investigation in MINOCA because it can exclude myocarditis, takotsubo syndrome, and cardiomyopathies, as well as provide imaging confirmation of AMI".9
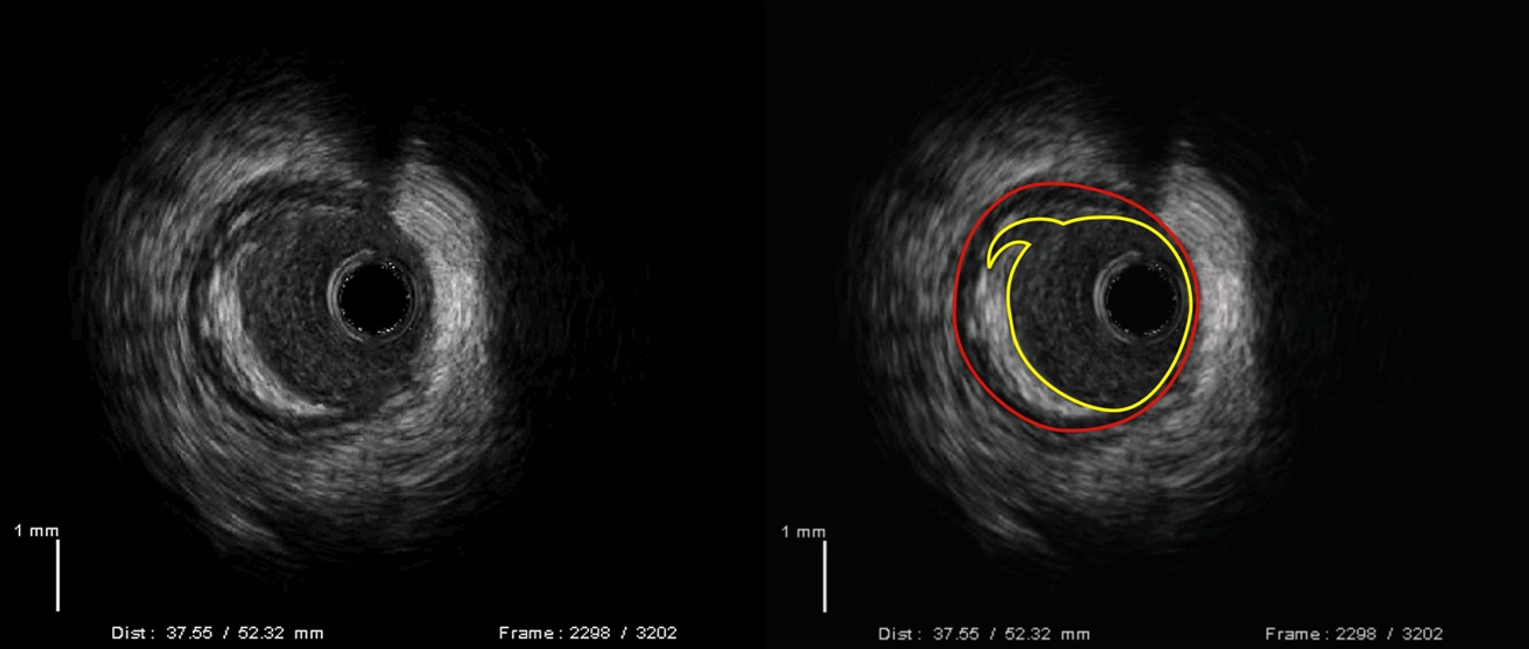
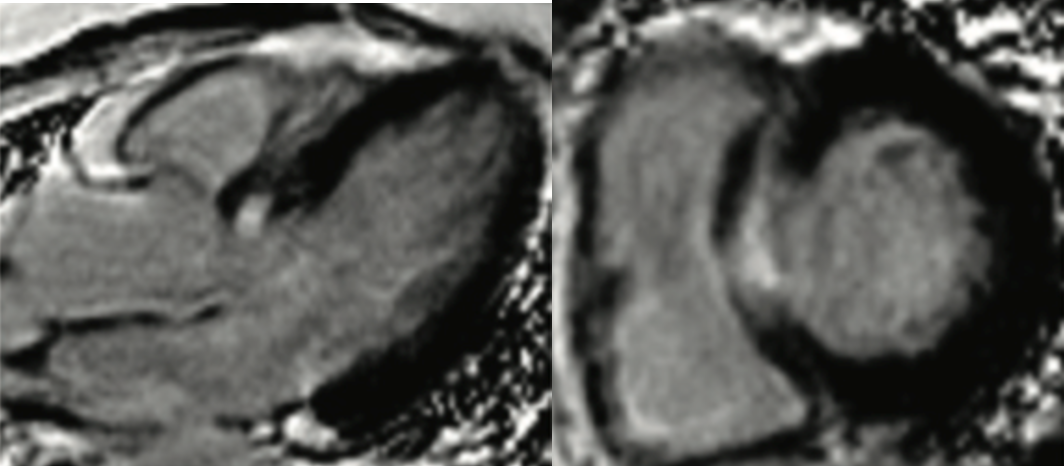
In this case, the patient underwent intracoronary imaging with IVUS, which revealed rupture of a nonobstructive atherosclerotic plaque in the proximal LAD (Figure 3). CMRI performed after angiography showed a transmural area of hyper-enhancement in the basal anterior interventricular septum on delayed enhancement images after administration of gadolinium contrast (Figure 4). The calculated LV ejection fraction by CMRI was 52%. In this case with a plaque rupture visualized by IVUS, CMRI was useful to confirm that the rupture was likely to be the cause of MI because the area of late gadolinium enhancement was observed in the territory supplied by the affected vascular segment.
Figure 3: IVUS With Plaque Rupture in the Proximal LAD
Figure 3
Figure 4
Figure 4
Subendocardial to transmural late gadolinium enhancement involving the basal anteroseptal wall is shown in the three-chamber and short-axis views. There was normal LV function.
Subendocardial to transmural late gadolinium enhancement involving the basal anteroseptal wall is shown in the three-chamber and short-axis views. There was normal LV function.
Coronary CT angiography (answer A) does not yet have sufficient luminal imaging resolution to reliably identify plaque disruption or subtle coronary artery dissection. However, it may be helpful to guide the need for statin therapy in patients with MINOCA who have normal lipid values if no atherosclerosis is observed by invasive coronary angiography. Single-photon emission CT myocardial perfusion imaging (answer C) would not provide any additional information on the mechanisms of MI. Intracoronary imaging alone (answer B) and CMRI alone (answer D) would not provide as much information as the two additional diagnostic tests in combination.
References
Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018;138:e618-e651.
Smilowitz NR, Mahajan AM, Roe MT, et al. Mortality of Myocardial Infarction by Sex, Age, and Obstructive Coronary Artery Disease Status in the ACTION Registry-GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry-Get With the Guidelines). Circ Cardiovasc Qual Outcomes 2017;10:e003443.
Reynolds HR, Srichai MB, Iqbal SN, et al. Mechanisms of myocardial infarction in women without angiographically obstructive coronary artery disease. Circulation 2011;124:1414-25.
Agewall S, Beltrame JF, Reynolds HR, et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J 2017;38:143-53.
Tamis-Holland JE, Jneid H, Reynolds HR, et al. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation 2019;139:e891-e908.
Smilowitz NR, Sampson BA, Abrecht CR, Siegfried JS, Hochman JS, Reynolds HR. Women have less severe and extensive coronary atherosclerosis in fatal cases of ischemic heart disease: an autopsy study. Am Heart J 2011;161:681-8.
Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation 2015;131:861-70.
vIqbal SN, Feit F, Mancini GB, et al. Characteristics of plaque disruption by intravascular ultrasound in women presenting with myocardial infarction without obstructive coronary artery disease. Am Heart J 2014;167:715-22.
Tamis-Holland JE, Jneid H, Reynolds HR, et al. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation 2019;139:e891-e908.