A 57-year-old female with a past medical history of viral pericarditis, atrial flutter and hypothyroidism presents with a 3-month history of progressive dyspnea on exertion, abdominal fullness and bilateral lower extremity edema.
She was initially diagnosed with viral pericarditis in 1988, for which she was treated with prednisone and indomethacin. She presented to an outside facility in 2012 complaining of abdominal pain. A right upper quadrant ultrasound was performed and showed a "portal vein abnormality" associated with small-to-moderate volume ascites. She was started on spironolactone and hydrochlorothiazide. She subsequently presented to pericardial clinic recently with profound shortness of breath with minimal exertion and bilateral lower extremity edema. Her electrocardiogram (Figure 1), chest x-ray (Figure 2), chest computed tomography (CT) (Figure 3) and echocardiogram Doppler images (Figures 4-6) are shown below.
Figure 1
Figure 1
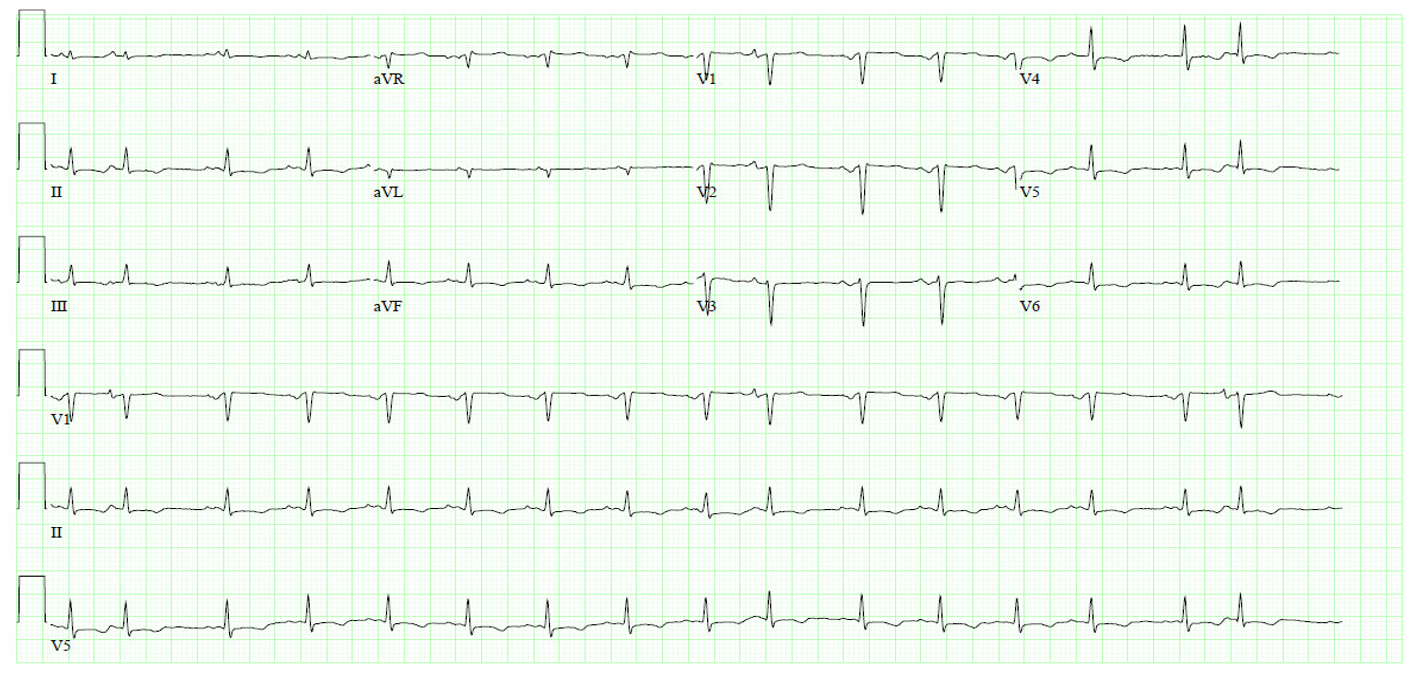
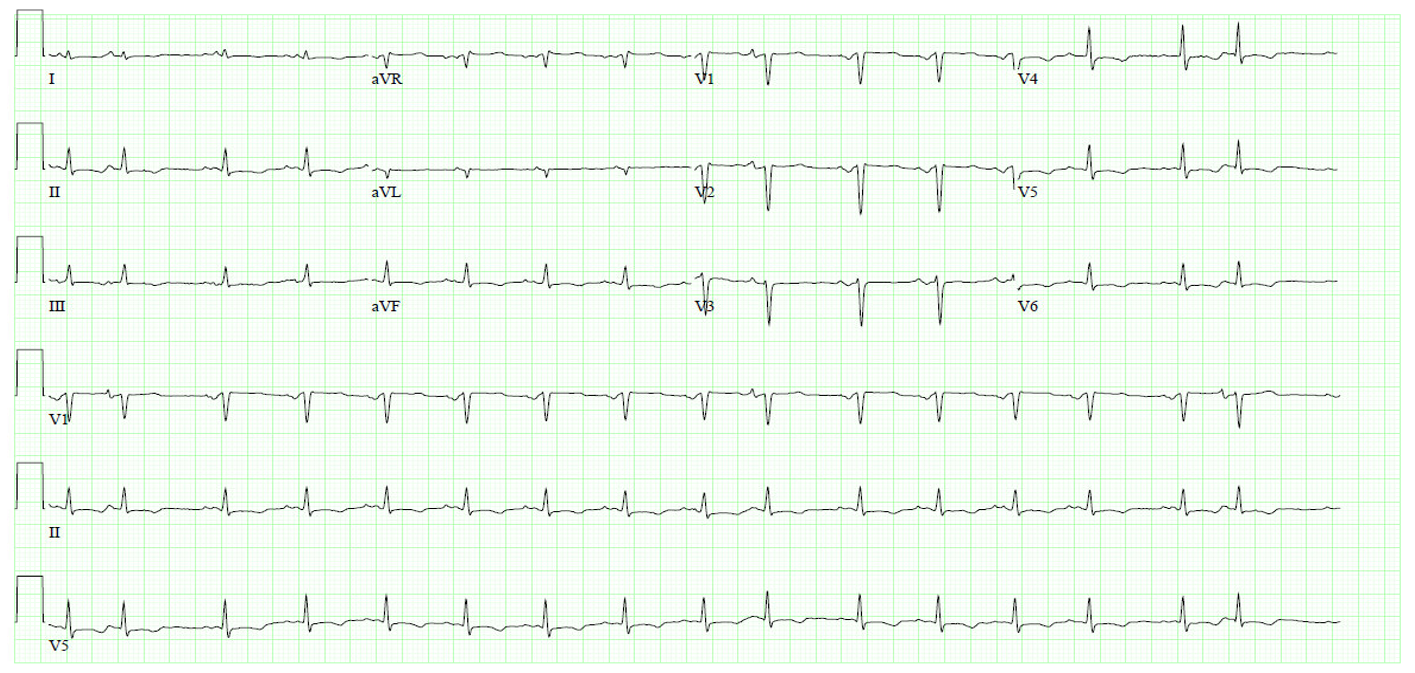
Figure 1: Electrocardiogram
Figure 1: Electrocardiogram
Figure 2
Figure 2
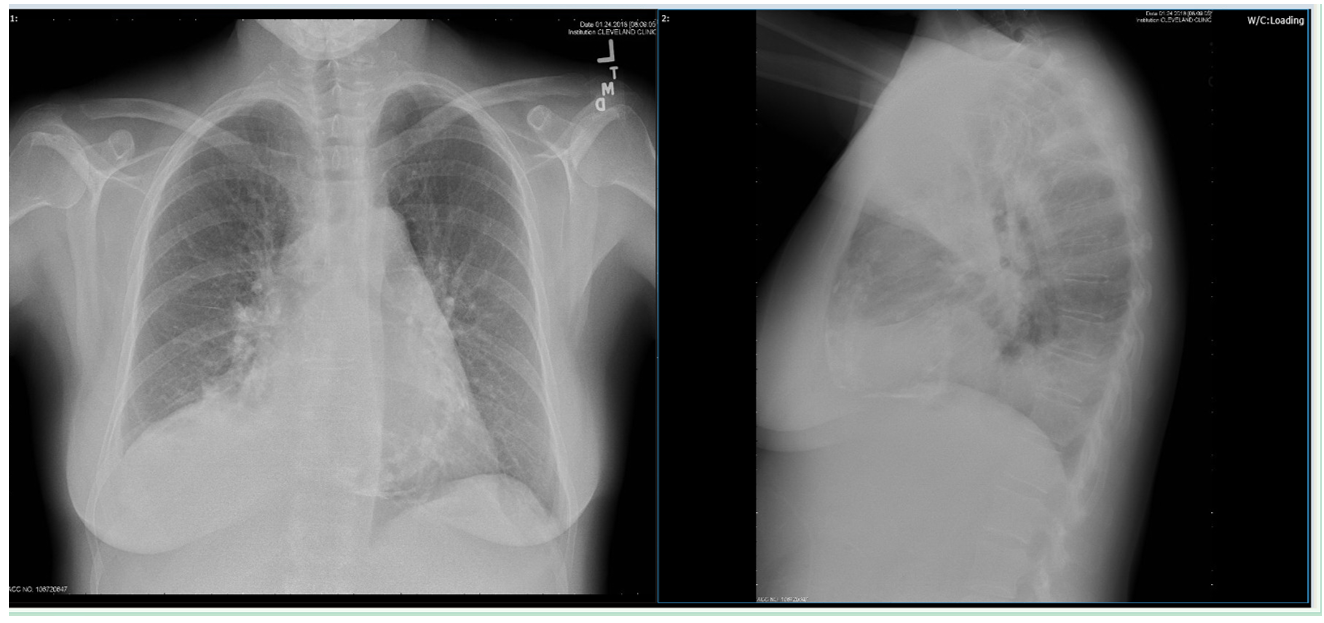
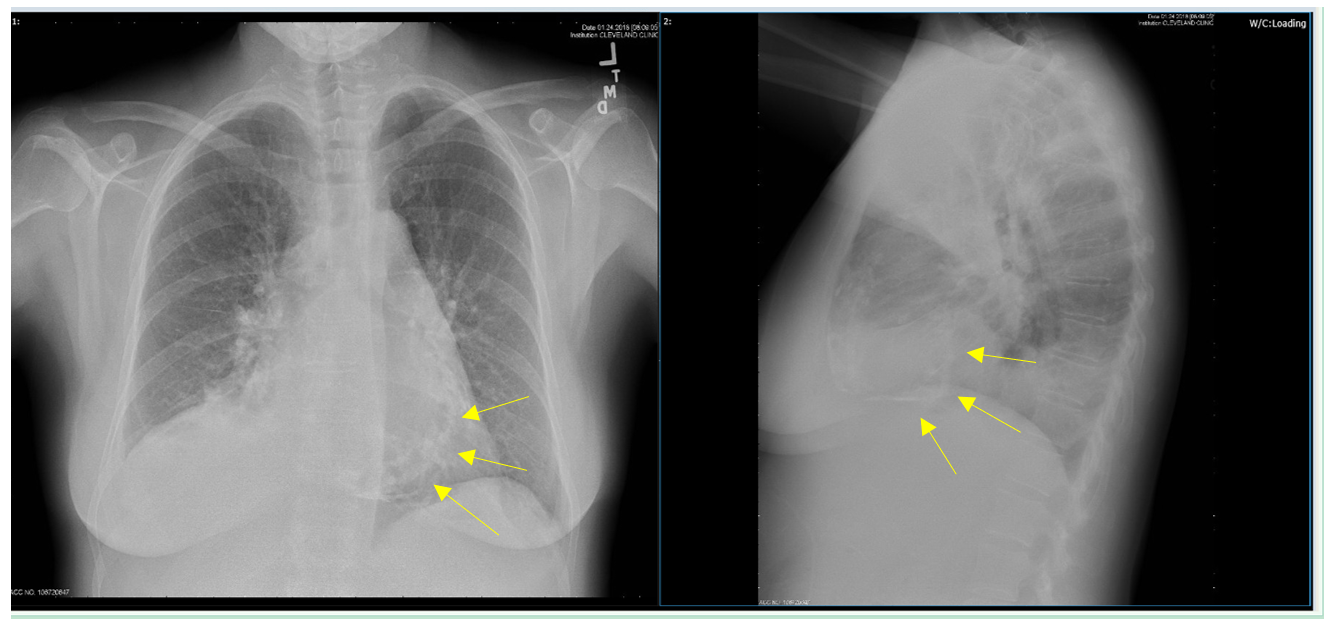
Figure 2: Chest x-ray
Figure 2: Chest x-ray
Figure 3
Figure 3
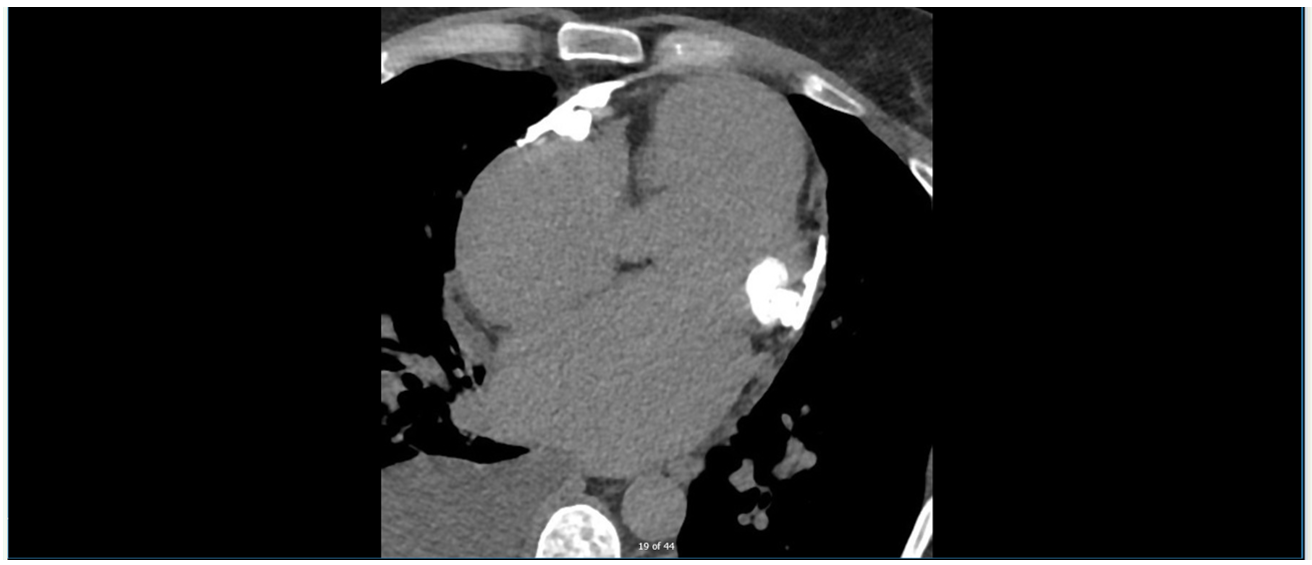
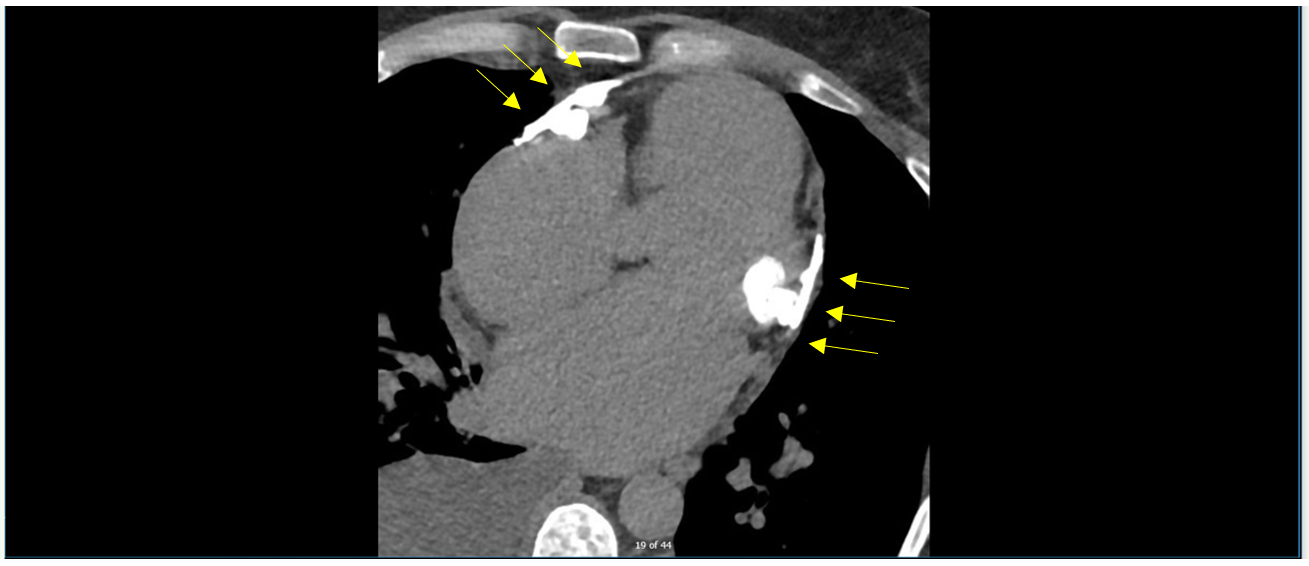
Figure 3: CT
Figure 3: CT
Figure 4
Figure 4
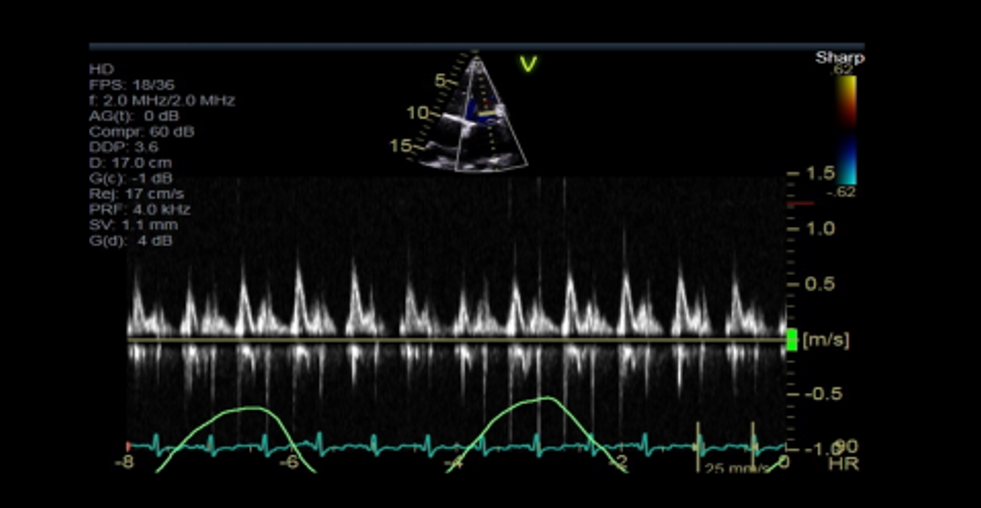
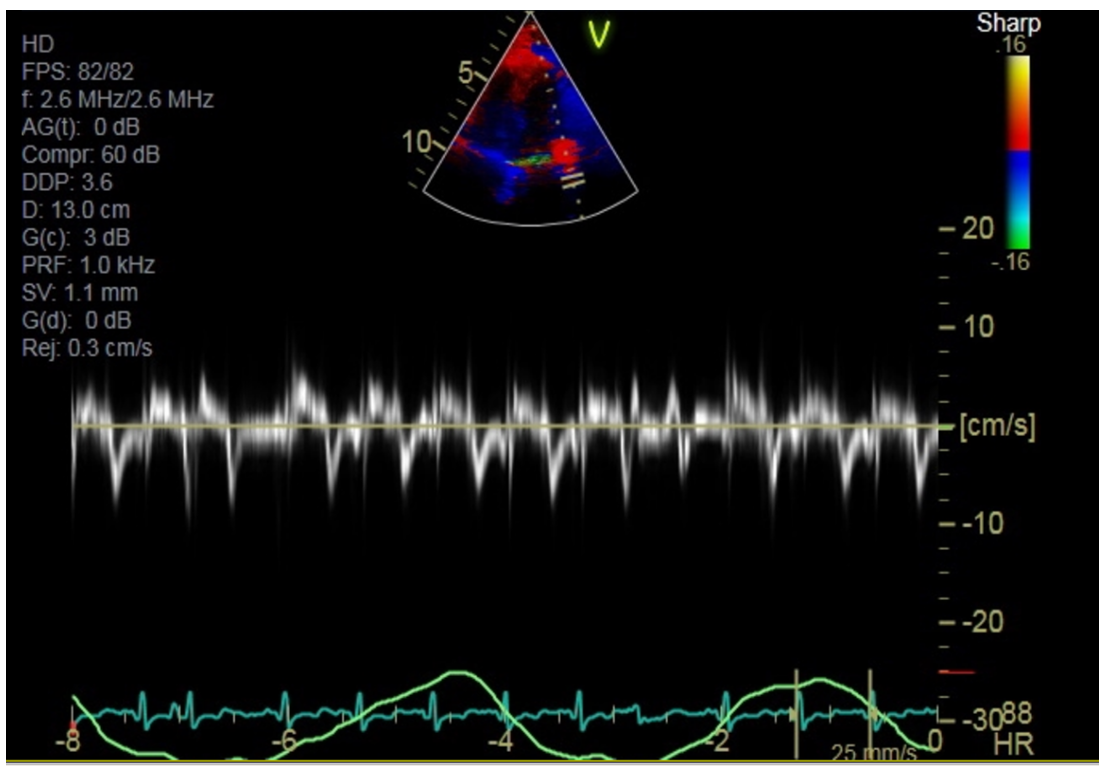
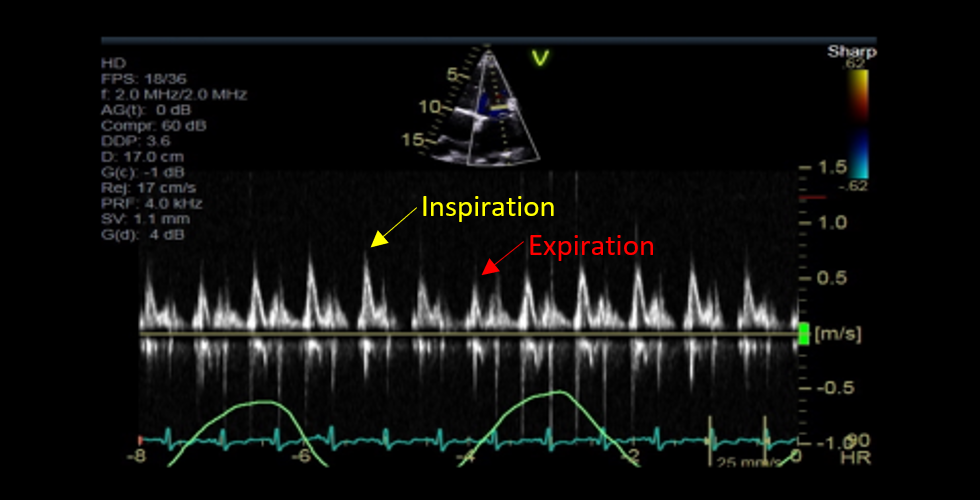
Figure 4: Pulse wave Doppler at the tips of the mitral valve with respirometer (green line)
Figure 4: Pulse wave Doppler at the tips of the mitral valve with respirometer (green line)
Figure 5
Figure 5
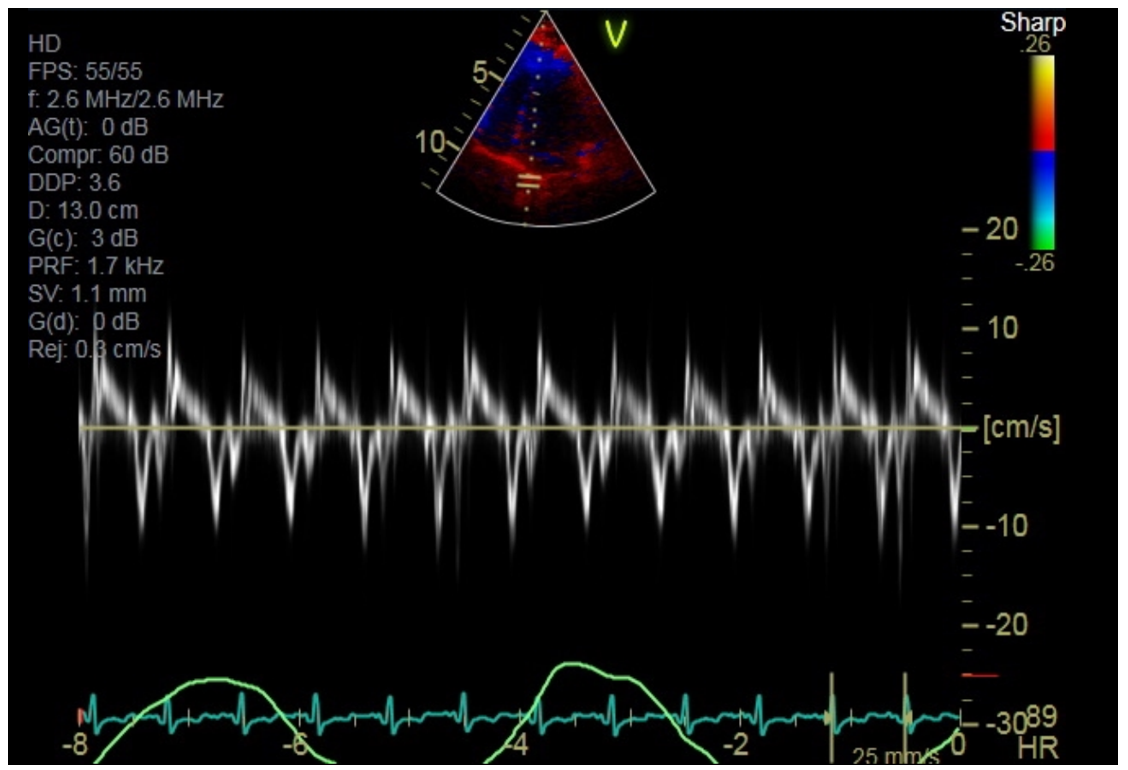
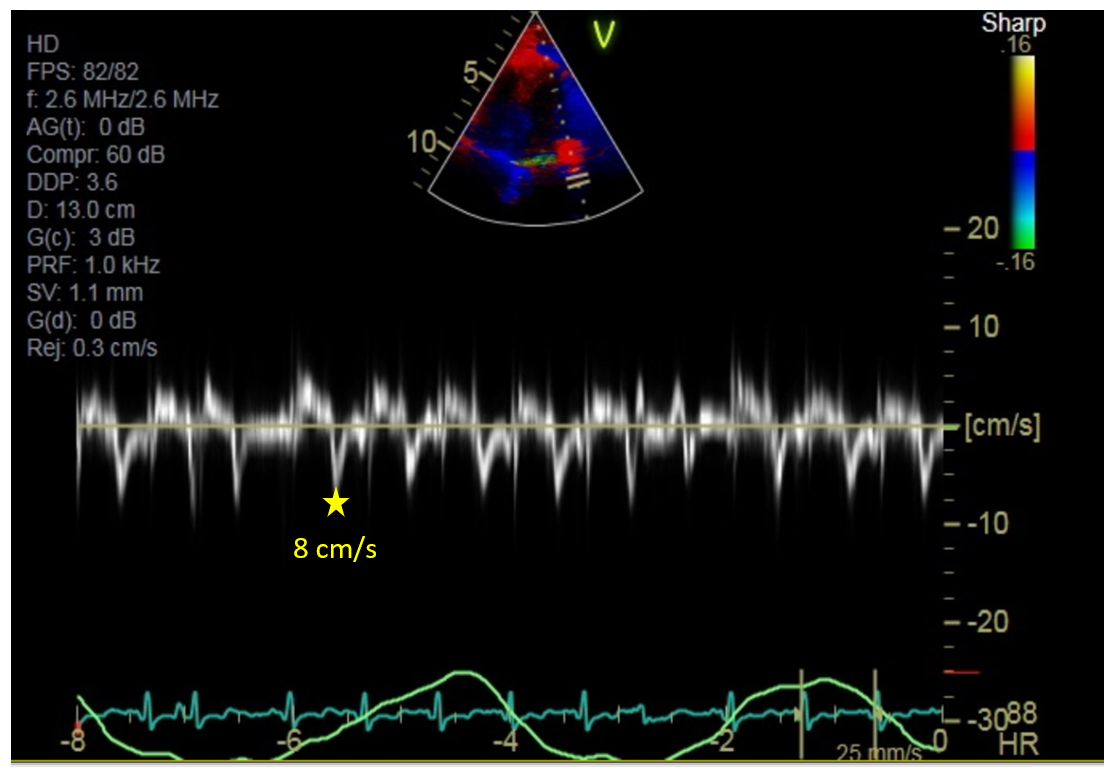
Figure 5: Tissue Doppler along the lateral aspect of the mitral valve annulus
Figure 5: Tissue Doppler along the lateral aspect of the mitral valve annulus
Figure 6
Figure 6
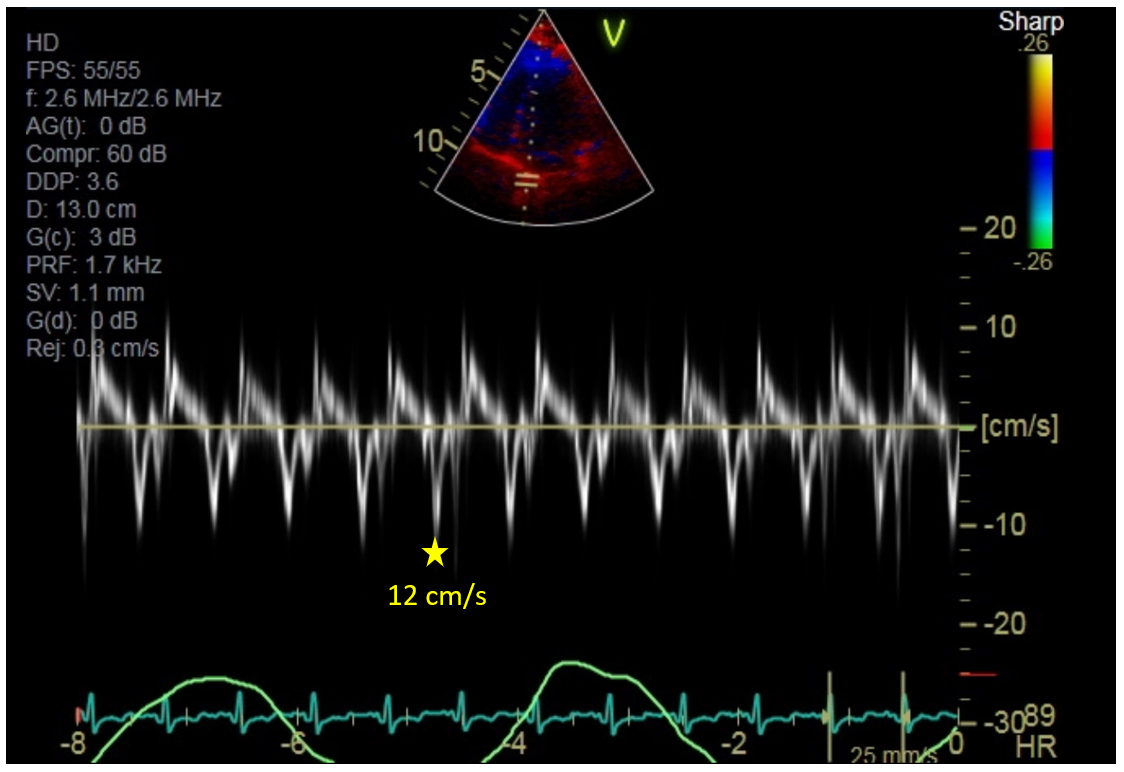
Figure 6: Tissue Doppler along the septal aspect of the mitral valve annulus
Figure 6: Tissue Doppler along the septal aspect of the mitral valve annulus
She underwent right heart catheterization which demonstrated the following: right atrial pressure 29 mmHg, right ventricular (RV) pressure 71/29 mmHg, pulmonary artery pressure 71/44 mmHg, pulmonary capillary wedge pressure of 30 mmHg, left ventricular (LV) pressure of 113/33 mmHg. Cardiac output was 2.8 L/min by Fick and 3.73 L/min by thermodilution. Her mixed venous oxygen saturation was 58%.
Which of the following findings on right heart catheterization would be the most specific for constrictive pericarditis?
Show Answer
The correct answer is: D. Systolic Area Index > 1.1
Given this patient's clinical history, their presentation is concerning for pericardial constriction. The patient's electrocardiogram has borderline low voltages in the limb leads (Figure 1A). The x-ray has a normal sized heart, however significant pericardial calcification can be seen, particularly along the atrioventricular groove (yellow arrows on Figure 2A). This pericardial calcification is confirmed on CT scan (yellow arrows on Figure 3A). Figure 4A shows respiratory variation of the mitral inflow velocity, suggestive of constriction. Figures 5A and 6A show mitral valve tissue Doppler velocities. Typically the velocity of the lateral e' is greater than the velocity of the septal e'. In pericardial constriction, the lateral mitral annulus is tethered to the pericardium, causing the lateral e' to be less than the septal e'. This is known as annulus reversus.1 In our scenario, the septal e' is approximately 12 cm/s, while the lateral e' is approximately 8 cm/s.
Figure 1A
Figure 1A
Figure 1A: Electrocardiogram. The precordial leads have borderline low voltages (< 5 mm).
Figure 1A: Electrocardiogram. The precordial leads have borderline low voltages (< 5 mm).
Figure 2A
Figure 2A
Figure 2A: Chest x-ray. Yellow arrows point to pericardial calcification.
Figure 2A: Chest x-ray. Yellow arrows point to pericardial calcification.
Figure 3A
Figure 3A
Figure 3A: CT. Yellow arrows point to pericardial calcification.
Figure 3A: CT. Yellow arrows point to pericardial calcification.
Figure 4A
Figure 4A
Figure 4A: Pulse wave Doppler at the tips of the mitral valve with respirometer. During inspiration (upward slope of the green line), there is decreased flow across the mitral valve (red arrow). During expiration (downward slope of the green line), there is increased flow across the mitral valve (yellow arrow).
Figure 4A: Pulse wave Doppler at the tips of the mitral valve with respirometer. During inspiration (upward slope of the green line), there is decreased flow across the mitral valve (red arrow). During expiration (downward slope of the green line), there is increased flow across the mitral valve (yellow arrow).
Figure 5A
Figure 5A
Figure 5A: Tissue Doppler along the lateral aspect of the mitral valve annulus. Septal e' is approximately 8 cm/s (yellow star).
Figure 5A: Tissue Doppler along the lateral aspect of the mitral valve annulus. Septal e' is approximately 8 cm/s (yellow star).
Figure 6A
Figure 6A
Figure 6A: Tissue Doppler along the septal aspect of the mitral valve annulus. Lateral e' is approximately 12 cm/s (yellow star).
Figure 6A: Tissue Doppler along the septal aspect of the mitral valve annulus. Lateral e' is approximately 12 cm/s (yellow star).
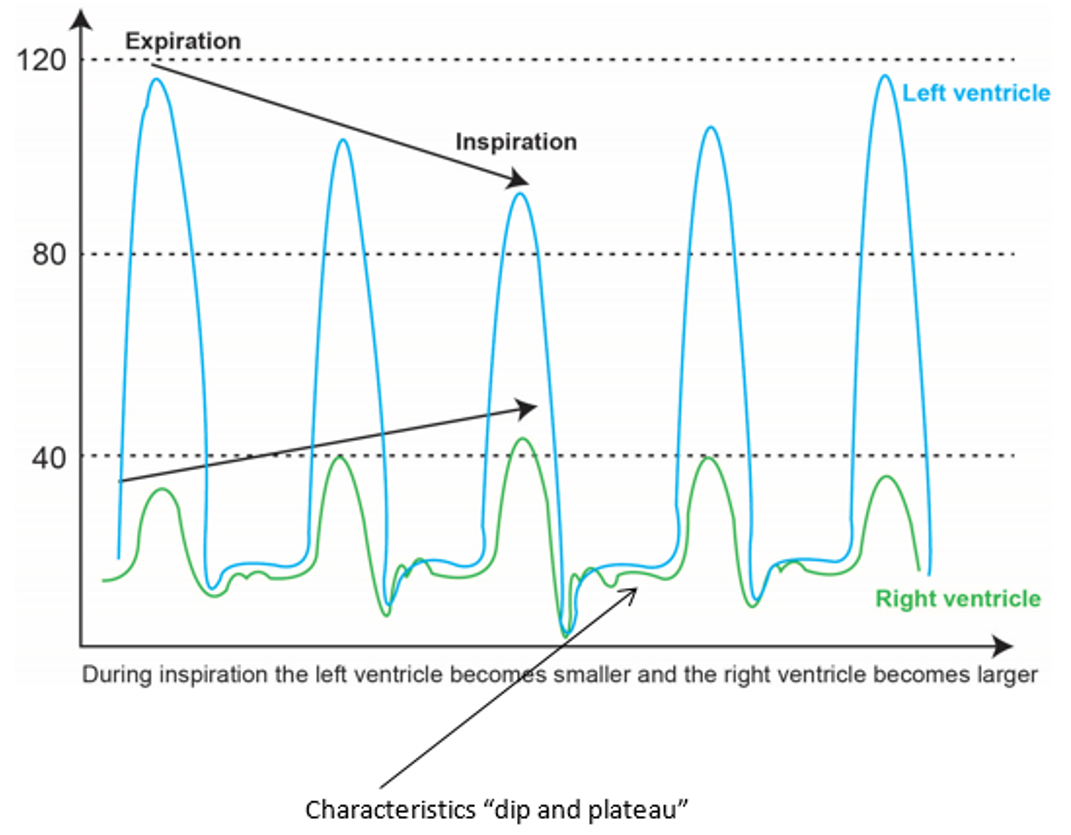
Invasive hemodynamics is commonly used in the diagnostic assessment of pericardial constriction. Characteristic findings include: increased right atrial pressure, prominent x and y descents on central venous and atrial tracings, increased right ventricular end diastolic pressure (RVEDP), "dip and plateau" waveform of the RV and LV diastolic pressure wave, and equalization of the LV and RV diastolic pressure. Inspiratory discordance of RV and LV pressure tracings is another pathognomonic finding of constriction (Figure 7).2
Figure 7
Figure 7
Figure 7: Pressure waveforms characteristic of pericardial constriction.
Figure 7: Pressure waveforms characteristic of pericardial constriction.
In order to distinguish cardiac restriction from constriction, further hemodynamic waveforms can be assessed. Talreja et al. studied intracardiac pressure waveforms in 100 consecutive patients undergoing right heart catheterization for constrictive pericarditis versus restrictive cardiomyopathy.3 Although there was a statistically significant difference when comparing the inspiratory decrease in right atrial pressure, difference between LVEDP and RVEDP, and the ratio of RVEDP/RV systolic pressure; there was overlap present for each of these criteria. With respect to the systolic area index, defined as the ratio of the RV area (mmHg x s) to the LV area (mmHg x s) in inspiration versus expiration, there was little overlap between those with constrictive pericarditis and restrictive cardiomyopathy (p<0.0001). On further analysis, the systolic area index had a 97% sensitivity and 100% specificity for the diagnosis of constrictive pericarditis.
References
Reuss CS, Wilansky SM, Lester SJ, et al. Using mitral 'annulus reversus' to diagnose constrictive pericarditis. Eur J Echocardiogr 2009;10:372-5.
Geske JB, Anavekar NS, Nishimura RA, Oh JK, Gersh BJ. Differentiation of constriction and restriction: complex cardiovascular hemodynamics. J Am Coll Cardiol 2016;68:2329-47.
Talreja DR, Nishimura RA, Oh JK, Holmes DR. Constrictive pericarditis in the modern era: novel criteria for diagnosis in the cardiac catheterization laboratory. J Am Coll Cardiol 2008;51:315-9.