In Fontan patients , CT scans performed to evaluate for thrombus may have significant artifact and must be interpreted in the context of flow dynamics.
Patients who undergo delayed primary Fontan operation are high risk and must be treated with a high suspicion for morbidity and complications when deviating from the expected course.
A procoagulant state exists in Fontan patients, especially in the first 6 months after the operation.
An 11-year-old male with dextrocardia, congenitally corrected transposition of the great arteries, subpulmonary stenosis, and a large inlet ventricular septal defect with a straddling tricuspid valve underwent primary non-fenestrated Fontan palliation due to exercise intolerance and cyanosis. He is on atenolol for a history of atrial tachycardia. His pre-Fontan cardiac catheterization demonstrated the following hemodynamics: indexed pulmonary vascular resistance (PVRi) 1.1 Wood.units.m2, cardiac index 2.9 L/min/m2, Qp:Qs ratio 0.6, aortic oxygen saturation 83%, left ventricle end-diastolic pressure 10 mmHg, and right ventricle end-diastolic pressure 11 mmHg. Upon weaning of bypass after his surgery, the central venous pressure measured 15 mmHg and the patient was extubated. A right internal jugular central line was removed 3 days later. His post-operative course was complicated by one episode of atrial tachycardia that resolved with initiation of his home dose of atenolol. He was started on 81 mg of acetylsalicylic acid daily. Between the fifth and eighth post-operative day, he required escalation of respiratory support and pain medications due to increased work of breathing and chest pain.
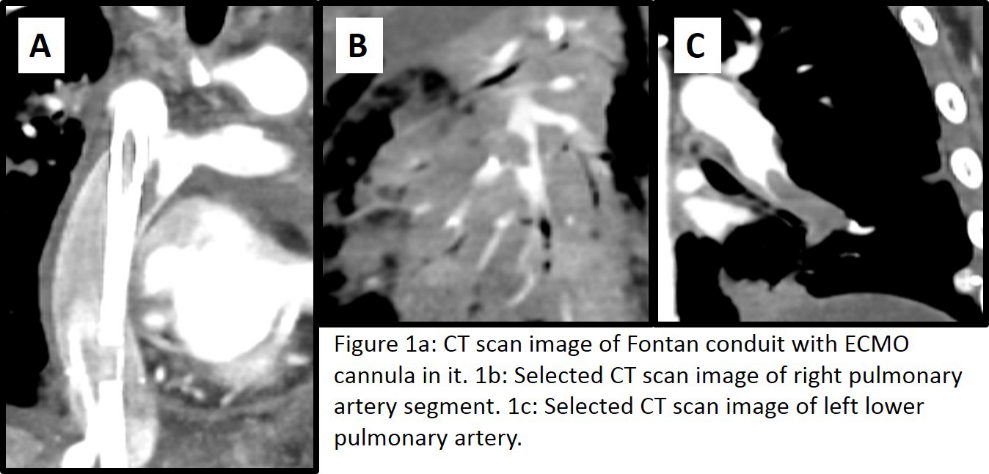
On the eighth post-operative day, the patient decompensated and required transfer to the intensive care unit (ICU). In the ICU, he arrested, and was intubated and cannulated for veno-arterial extracorporeal membrane oxygenation (ECMO) via the right internal jugular vein and carotid artery. Once stabilized on ECMO, a chest computed tomography (CT) scan was obtained (Figure 1). Notably, factor 8 was 185 (high) and von Willebrand factor antigen was >400 (high) immediately after ECMO cannulation.
Figure 1
Figure 1
What was the most likely cause of this patient's decompensation?
Show Answer
The correct answer is: C. Multiple pulmonary artery thromboses
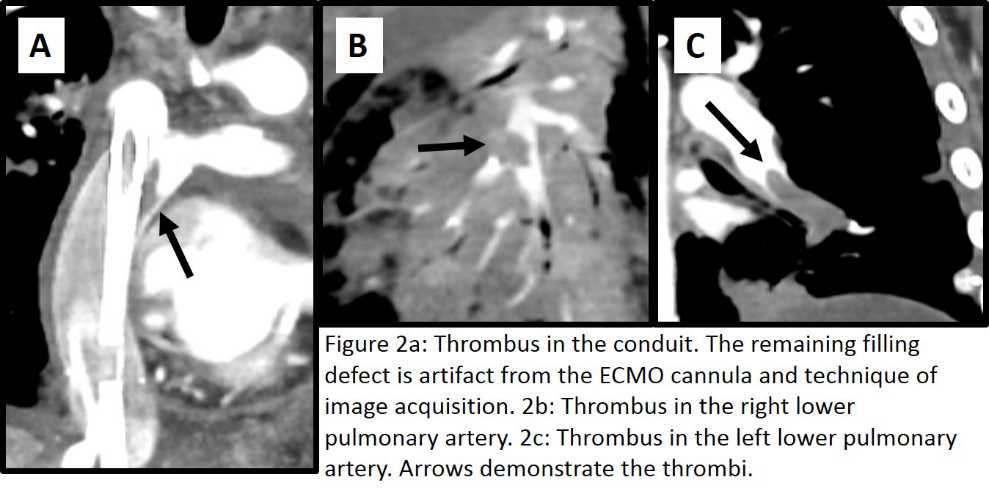
The most likely cause of this patient's decompensation is C. Multiple pulmonary artery thromboses. Thromboses in the distal right pulmonary artery and the distal left pulmonary artery can be seen in the CT Scan (Figure 2).
Figure 2
Figure 2
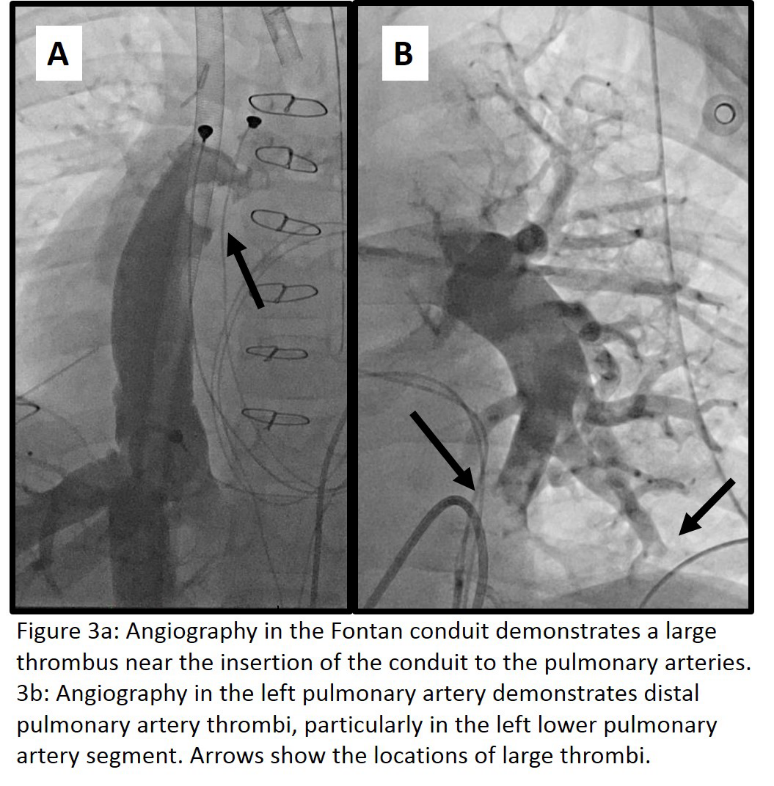
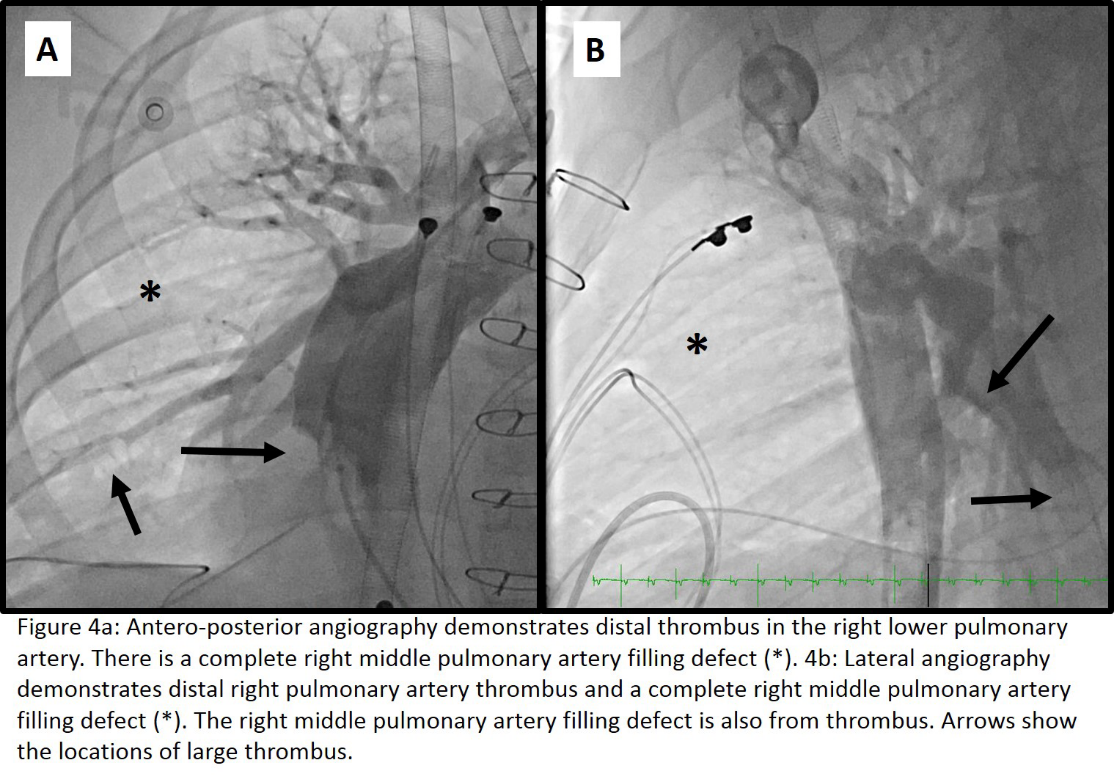
The multiple thromboses caused this patient to lose nearly all forward flow through the passive Fontan system and therefore lose cardiac output. The CT Scan also demonstrates an unobstructive thrombus on the ECMO cannula in the Fontan conduit. While the imaging appears concerning for extensive conduit thrombosis, this was actually artifact. Artifact in the conduit and pulmonary arteries on CT scans is common in Fontan patients due to altered anatomy and hemodynamics. Injection of contrast material from one upper or lower extremity can lead to a mixture of opacified and unopacified blood that can resemble thrombosis. In order to prevent this error, simultaneous injections of contrast in both the upper and lower extremity with image acquisition in the early and delayed phases of contrast enhancement is recommended.1 Extensive pulmonary thromboses were demonstrated with angiography during catheterization performed for mechanical thrombectomy and placement of catheters for ultrasound-assisted catheter-directed thrombolysis with tissue plasminogen activator (Figures 3 and 4).
Figure 3
Figure 3
Figure 4
Figure 4
There is an increased rate of thromboembolic complications in older Fontan patients with atrial arrhythmias,2 but this is unlikely in this patient because the patient's atrial tachycardia was well controlled on atenolol. This patient had normal PVRi, making a pulmonary hypertension crisis from elevated PVRi an unlikely cause of decompensation. Deep vein thrombosis with an embolic event to the Fontan conduit and pulmonary arteries is possible. However, the patient had lower extremity ultrasounds demonstrating no thromboses.
Fontan patients have a general pro-thrombotic state after the operation.2-10 An international, multicenter study found that factors associated with thrombosis included underlying pulmonary atresia with intact ventricular septum, pulmonary artery distortion, lower pre-operative unconjugated bilirubin, use of central venous lines for more than 10 days or until hospital discharge, and lower fraction of inspired oxygen 24 hours after the Fontan procedure. Patients who consistently met the target international normalized ratio (INR) levels while on warfarin or who were on acetylsalicylic acid had a 3.5 fold decreased risk of thrombosis compared to patients who did not meet the target INR levels. Many studies have demonstrated that factor 8 is increased and protein C decreased after the Fontan procedure.5,8,9 Some have attributed the increase in coagulation abnormalities to temporary liver dysfunction and others have attributed elevated von Willebrand factor levels to the endothelial dysfunction found in a Fontan circuit.9,11,12 Our patient had both elevated factor 8 and von Willebrand factor levels.
This patient underwent a primary Fontan procedure rather than a staged palliation. The primary Fontan procedure results in acute volume unloading and can be poorly tolerated.13 A single center retrospective review demonstrated 11 of 105 patients (10.5%) with early deaths within a median of 10 days after surgery and 24 of 94 (25.5%) had early morbidity, including two with thromboembolic events.14 An additional single center study evaluating primary Fontan patients over 15 years of age found 2 of 88 patients with mortality from pulmonary emboli.15
Our patient received mechanical thrombectomy in the catheterization lab for three consecutive days. In addition, the patient received 3 days of ultrasound assisted catheter directed thrombolysis. The Fontan was taken down and a 10 mm central shunt placed. The patient was able to be decannulated from ECMO and extubated. He had a prolonged hospital course due to deconditioning, renal insufficiency, and stroke. He underwent rehabilitation and was discharged home, demonstrating no neurologic sequelae, renal recovery, minimal oxygen requirement, and improved exercise tolerance. At this time, there are no plans for further surgical interventions.
References
Mahani MG, Agarwal PP, Rigsby CK, et al. CT for assessment of thrombosis and pulmonary embolism in multiple states of single-ventricle palliation: challenges and suggested protocols. Radiographics 2016;36:1273-84.
Egbe AC, Connolly HM, McLeod CJ, et al. Thrombotic and embolic complications associated with atrial arrhythmia after Fontan operation: role of prophylactic therapy. J Am Coll Cardiol 2016;68:1312-9.
Egbe AC, Connolly HM, Niaz T, et al. Prevalence and outcome of thrombotic and embolic complications in adults after Fontan operation. Am Heart J 2017;183:10-7.
Grewal J, Al Hussein M, Feldstein J, et al. Evaluation of silent thrombus after the Fontan operation. Congenit Heart Dis 2013;8:40-7.
Jahangiri M, Kreutzer J, Zurakowski D, Bacha E, Jonas RA. Evaluation of hemostatic and coagulation factor abnormalities in patients undergoing the Fontan operation. J Thorac Cardiovasc Surg 2000;120:778-82.
McCrindle BW, Manlhiot C, Cochrane A, et al. Factors associated with thrombotic complications after the Fontan procedure: a secondary analysis of a multicenter, randomized trial of primary thromboprophylaxis for 2 years after the Fontan procedure. J Am Coll Cardiol 2013;61:346-53.
Odegard KC, Zurakowski D, DiNardo JA, et al. Prospective longitudinal study of coagulation profiles in children with hypoplastic left heart syndrome from stage I through Fontan completion. J Thorac Cardiovasc Surg 2009;137:934-41.
Odegard KC, McGowan FX Jr, Zurakowski D, et al. Procoagulant and anticoagulant factor abnormalities following the Fontan procedure: increased factor VIII may predispose to thrombosis. J Thorac Cardiovasc Surg 2003;125:1260-7.
Procelewska M, Kolcz J, Januszewska K, Mroczek T, Malec E. Coagulation abnormalities and liver function after hemi-Fontan and Fontan procedures – the importance of hemodynamics in the early postoperative period. Eur J Cardiothorac Surg 2007;31:866-72.
Varma C, Warr MR, Hendler AL, Paul NS, Webb GD, Therrien J. Prevalence of "silent" pulmonary emboli in adults after the Fontan operation. J Am Coll Cardiol 2003;41:2252-8.
Henaine R, Vergnat M, Bacha EA, et al. Effects of lack of pulsatility on pulmonary endothelial function in the Fontan circulation. J Thorac Cardiovasc Surg 2013;146:522-9.
Binotto MA, Maeda NY, Lopes AA. Altered endothelial function following the Fontan procedure. Cardiol Young 2008;18:70-4.
Gibson PH, Burns JE, Walker H, Cross S, Leslie SJ. Keeping track of congenital heart disease – is it time for a national registry? Int J Cardiol 2010;145:331-2.
Talwar S, Singh S, Sreenivas V, et al. Outcomes of patients undergoing primary Fontan operation beyond first decade of life. World J Pediatr Congenit Heart Surg 2017;8:487-94.
Valente AM, Lewis M, Vaziri SM, et al. Outcomes of adolescents and adults undergoing primary Fontan procedure. Am J Cardiol 2013;112:1938-42.