A 77-year-old male presents to outpatient clinic with chronic dyspnea on exertion (NYHA Class II symptoms), lower extremity swelling, and intermittent chest pain on exertion. He describes his chest discomfort as occasionally pleuritic and non-positional. Past medical history includes coronary artery disease (CAD) status-post multiple stents, chronic diastolic heart failure, permanent atrial fibrillation with two failed cardioversions, hypertension, hyperlipidemia, and type II diabetes mellitus. He has worked in a paper mill for many years.
The chest pain began in 2017 with associated nasal congestion. He presented to a local hospital and was diagnosed with new onset right sided pleural effusion. He underwent thoracentesis with recurrence of effusion in 3-4 months. He was subsequently discovered to have interstitial lung disease and calcified pleural plaque related to asbestos exposure.
On exam, he was in no acute distress. He had a positive jugular venous distention and positive Kussmaul's sign. He had decreased breath sounds at right lung base without any wheezing or crackles. Pulse was irregularly irregular with a diastolic murmur and a pericardial knock. He also had 2+ bilateral pitting edema.
Labs showed: normal complete blood count and normal comprehensive metabolic panel. Erythrocyte sedimentation rate (ESR) was 28 which was slightly elevated.
Figure 1
Figure 1
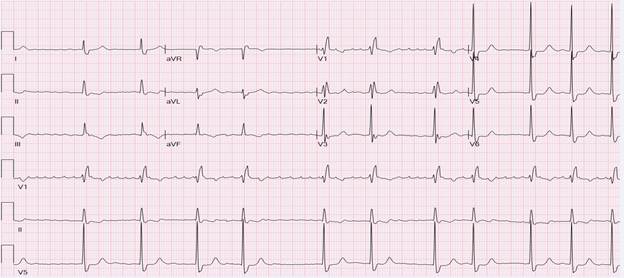
Figure 1: ECG showed rate atrial fibrillation with a right bundle branch block.
Figure 1: ECG showed rate atrial fibrillation with a right bundle branch block.
Video 1
Video 1
Video 1: On echocardiography, apical four chamber view showing diastolic septal bounce.
Video 1: On echocardiography, apical four chamber view showing diastolic septal bounce.
Figure 2A
Figure 2A
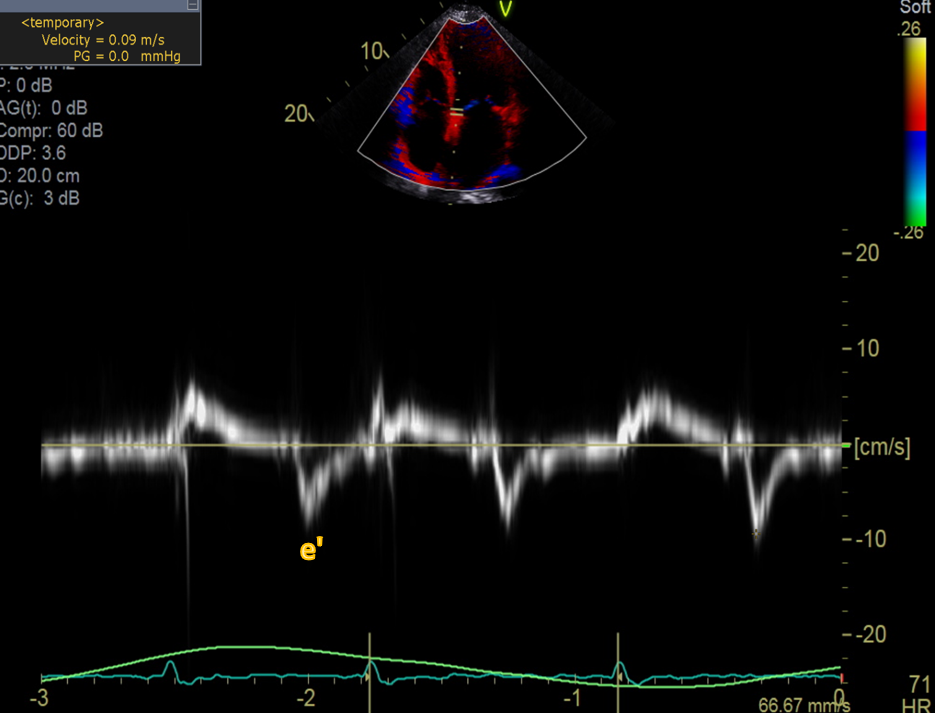
Figure 2(A-B): Doppler echocardiography showing early diastolic mitral annulus velocity (e') estimated by tissue doppler (TD). Tissue doppler – lateral e' 6cm/s (A), septal e' 9 cm/s (B) suggesting annulus reversus, where septal e' is greater than lateral e' as the lateral annular excursion is limited by the abnormal pericardium in constrictive pericarditis. Normally the lateral e' is greater than the septal e' velocity.
Figure 2B
Figure 2B
Figure 2(A-B): Doppler echocardiography showing early diastolic mitral annulus velocity (e') estimated by tissue doppler (TD). Tissue doppler – lateral e' 6cm/s (A), septal e' 9 cm/s (B) suggesting annulus reversus, where septal e' is greater than lateral e' as the lateral annular excursion is limited by the abnormal pericardium in constrictive pericarditis. Normally the lateral e' is greater than the septal e' velocity.
Figure 2(A-B): Doppler echocardiography showing early diastolic mitral annulus velocity (e') estimated by tissue doppler (TD). Tissue doppler – lateral e' 6cm/s (A), septal e' 9 cm/s (B) suggesting annulus reversus, where septal e' is greater than lateral e' as the lateral annular excursion is limited by the abnormal pericardium in constrictive pericarditis. Normally the lateral e' is greater than the septal e' velocity.
Figure 3
Figure 3
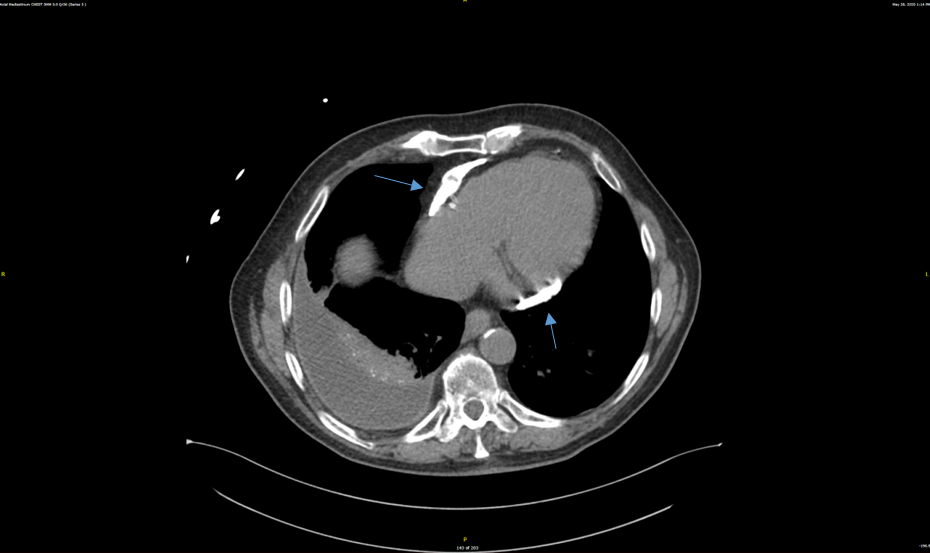
Figure 3: Chest computed tomography showing coarse calcifications of the pericardium and right sided pleural effusion.
Figure 3: Chest computed tomography showing coarse calcifications of the pericardium and right sided pleural effusion.
What is the best recommended next step in management?
Show Answer
The correct answer is: D. Radical pericardiectomy
This patient's clinical history, exam, and imaging findings are consistent with chronic constrictive pericarditis. In constrictive pericarditis, dense fibrous thickening of the pericardium impairs diastolic filling of the heart which manifests as venous congestion and diminished cardiac output.1 Etiologies include idiopathic or viral (42-61%), post-cardiac surgery (11-37%), post-radiation therapy, connective tissue disorders, post-infectious, and other causes such as malignancy, trauma, tuberculosis, asbestosis, sarcoidosis, and uremia.2
Constrictive pericarditis has a progressive but variable course. There are four different phenotypes of pericarditis which include acute (+/- possible transient constrictive physiology) recurrent (+/- subacute or effusive constriction), chronic and burned-out or calcific constrictive pericarditis. For most patients with calcific or burned-out pericarditis, surgical pericardiectomy is the definitive treatment.3 Healthy elderly patients with very mild constriction may be managed non-surgically, with pericardiectomy deferred until the disease progresses. Patients with major comorbidities and/or severe debilitation may be at too high a risk for pericardiectomy. Radiation-induced disease is considered a relative contraindication. Otherwise, surgery should ordinarily not be delayed once the diagnosis is made.
There is a strong association between the presumed etiology of constrictive pericarditis and post-pericardiectomy outcomes.4 Patients with idiopathic disease had excellent outcomes whereas patients with post-radiation disease had significantly worse overall survival.4 The effects of radiation on cardiac structures, including premature CAD, cardiomyopathy with mixed restrictive and constrictive disease, and valvular abnormalities are likely to have an adverse impact on perioperative mortality as well as survival. Independent predictors of death include radiation induced heart disease, impaired renal function, abnormal LV systolic function, lower sodium levels, and older age.4-6
Studies have also assessed calcium burden on computed tomography (CT) imaging and outcomes in patients with constrictive pericarditis. A retrospective study by Senapati et al. evaluated the pattern of pericardial calcium distribution by CT in constrictive pericarditis using semiquantitative calcium scoring system to calculate total pericardial calcium burden and distribution.7 Preferential distribution of calcium in a partial band-line pattern from basal anterolateral LV going inferiorly and then encircling the heart to reach the RV outflow tract with extension into mitral and tricuspid annuli was noted. There was no significant difference in adverse surgical outcomes or all-cause mortality between the calcified and non-calcified pericardium groups. Higher diuretic use, incidence of atrial fibrillation, COPD and larger atrial as well as inferior vena cava (IVC) diameters were found in the calcified pericardium group.7
Diuretics and salt restriction are useful for relief of volume overload, but some patients with constrictive pericarditis ultimately become refractory to medical management. Because sinus tachycardia is a compensatory mechanism, beta-adrenergic blockers and calcium channel antagonists that slow the heart rate may be poorly tolerated; if initiated, clinical response should be closely monitored. Anti-inflammatory agents may be initiated if there are signs of active inflammation, however for patients with persisting evidence of constriction like the patient in this case, pericardiectomy is advised.8
References
Mehta A, Mehta M, Jain AC. Constrictive pericarditis. Clin Cardiol 1999;22:334-44.
Adler Y, Charron P, Imazio M, et al. The 2015 ESC guidelines on the diagnosis and management of pericardial diseases. Eur Heart J 2015;36:2921-64.
Chetrit M, Xu B, Kwon DH, et al. Imaging-guided therapies for pericardial diseases. JACC Cardiovasc Imaging 2020;13:1422-37.
Bertog SC, Thambidorai SK, Parakh K, et al. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol 2004;43:1445-52.
Inamdar KY, Aikebaier M, Lijunhong, Abudunaibi, Mulati A. Pericardiectomy: prompt surgical management of constrictive pericarditis. Heart Surg Forum 2014;17:E319-22.
Unai S, Johnston DR. Radical pericardiectomy for pericardial diseases. Curr Cardiol Rep 2019;21:6.
Senapati A, Isma'eel HA, Kumar A, et al. Disparity in spatial distribution of pericardial calcifications in constrictive pericarditis. Open Heart 2018;5:e000835.
Clare GC, Troughton RW. Management of constrictive pericarditis in the 21st century. Curr Treat Options Cardiovasc Med 2007;9:436-42.