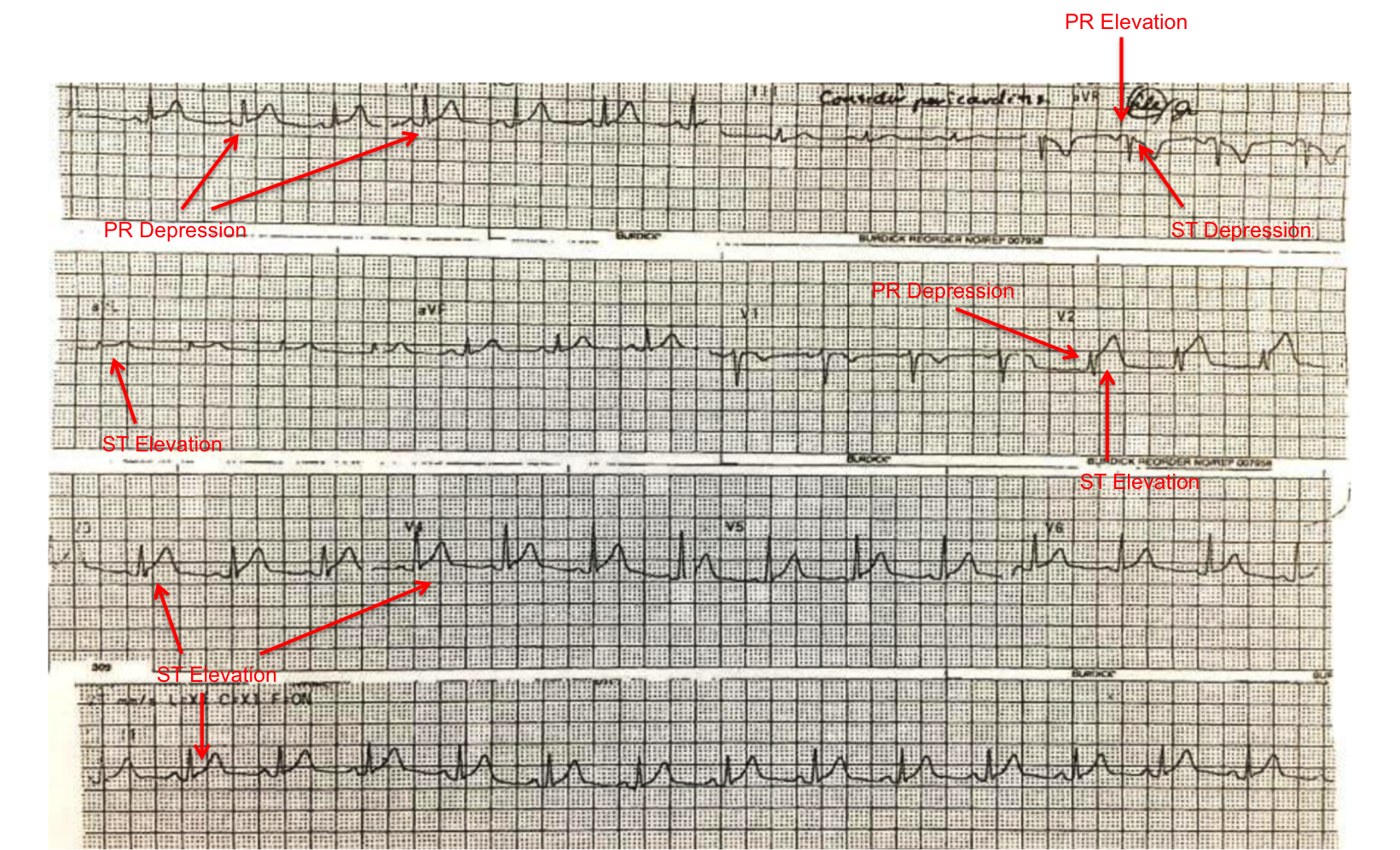
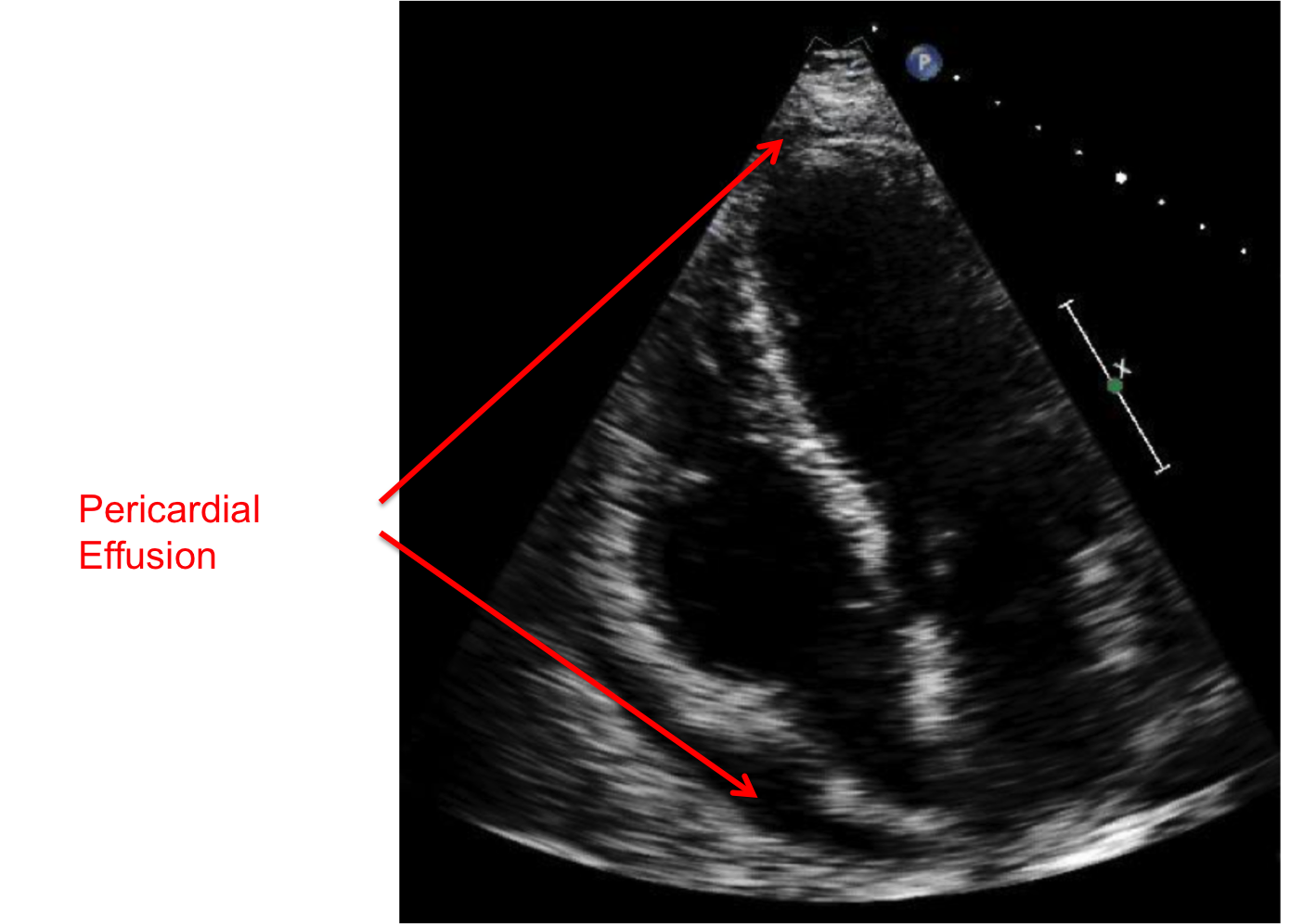
A 62-year-old male physician with a history of well-controlled gastroesophageal reflux disease and hypothyroidism presents for evaluation of recurrent, pleuritic chest pain that was worse with deep inspiration and lying flat. He first presented to his primary care provider months ago with dyspnea, fevers and fatigue. Electrocardiogram showed diffuse ST segment elevations and PR depressions (Figure 1). On physical exam, his BP was 122/75, heart rate of 70 beats per minute, temperature of 37.1°C, respiratory rate of 14 per minute, and oxygen saturation of 97% on room air. His jugular venous pressure was not elevated at 45 degrees. Cardiac exam revealed a normal S1 and S2 with no additional heart sounds and did not reveal a pericardial rub. Erythrocyte sedimentation rate was 38 mm/hr and C-reactive protein was 5.2 mg/L. Echocardiogram at the time showed a small circumferential pericardial effusion without signs of tamponade (Figure 2). The patient diagnosed himself with acute pericarditis and began treatment with oral prednisone 40 mg daily. Over the past several months he has tried several quick tapers off of prednisone without complete resolution of his symptoms and started on colchicine two months ago.
Figure 1: Rhythm strip showing diffuse ST-elevations and PR depressions with PR elevation and ST-depression in a lead aVR.
Figure 2: Transthoracic echocardiogram: apical four chamber view showing a small, circumferential pericardial effusion.
Which of the following is the patient's diagnosis and most appropriate treatment strategy?
Show Answer
The correct answer is: D. Incessant pericarditis' triple therapy with the addition of a nonsteroidal anti-inflammatory and continue prednisone and colchicine with a prolonged taper over several months.
This patient meets diagnostic criteria for acute pericarditis which is defined by at least two of the following four criteria: pericarditic chest pain, pericardial rub, new widespread ST-elevation or PR depression on electrocardiogram, or a pericardial effusion that is new or worsening. His acute pericarditis is best defined as incessant pericarditis. Unlike acute pericarditis, incessant pericarditis is defined as pericarditis lasting for >4-6 weeks but <3 months without remission. Recurrent pericarditis is defined as recurrence of pericarditis after a documented first episode of acute pericarditis and a symptom-free interval of 4-6 weeks or longer. Chronic pericarditis is pericarditis lasting for >3 months.1,2 Treatment guidelines for acute pericarditis include restriction of physical activity beyond an ordinary sedentary lifestyle until symptom resolution and normalization of C-reactive protein (at least 3 months).1 Aspirin by mouth at a dose of 750-1000mg every 8 hours or other nonsteroidal anti-inflammatory (e.g., ibuprofen 600mg by mouth every 8 hours) are the mainstays of therapy for acute pericarditis. Nonsteroidal anti-inflammatories are tapered every 1-2 weeks. Colchocine is recommended at a low, weight-adjusted dose (0.5mg by mouth once daily if <70kg or 0.5mg by mouth twice daily if ≥70kg) for 3 months to improve responses to medical therapy and prevent recurrences.1,2 In uncomplicated acute idiopathic pericarditis, glucocorticoids should not be used as a primary therapy as they are associated with high rates of relapse when stopped or tapered and blunt the efficacy of colchicine in preventing recurrences. Glucocorticoids should not be started if a patient presents with recurrence of symptoms without objective findings. Glucocorticoids at low to moderate doses (e.g., prednisone 0.2 to 0.5 mg/kg/day) can be considered as a second option in patients with contraindications and failure of aspirin or nonsteroidal anti-inflammatories. Very slow tapering is recommended especially in recurrent cases.1,2,4
References
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and managemetn of pericardial diseases: the Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA 2015;314:1498-506.
Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis. N Engl J Med 2013;369:1522-8.
Cremer PC, Kumar A, Kontzias A, et al. Complicated pericarditis: understanding risk factors and pathophysiology to inform imaging and treatment. J Am Coll Cardiol 2016;68:2311-28.