A 39-year-old male patient without any previous medical history presented to a peripheral hospital's emergency department with an acute onset of confusion. The confusion was preceded by a flu-like prodrome followed by persistent fevers and periodic chest discomfort. Initial investigations yielded an abnormal lumbar puncture and streptococcal bacteremia. His initial electrocardiogram (ECG) showed sinus tachycardia, and his peak troponin I was 0.291 mcg/L along with a C-reactive protein of 228.1 mg/L.
The patient was promptly started on intravenous antibiotics for meningitis. Investigations for the source of bacteremia were initiated, including a transthoracic echocardiogram (TTE) that showed a left ventricular ejection fraction of 60-65% and moderately increased pulmonary pressures of 48 mmHg. Also noted was a heavily calcified and moderately stenotic aortic valve (peak-to-mean pressure gradient 53/35 mmHg, dimensionless index 0.37, aortic valve area 1.43 cm2). No vegetation was identified. The surface echocardiogram was followed by a transesophageal echocardiogram (TEE) that confirmed the former and identified mild-to-moderate aortic insufficiency but, again, could not identify a vegetation nor any obvious complication of infective endocarditis (IE).
Following several days of intravenous antibiotics, the patient's clinical status improved, including sterilization of the blood cultures. Fever and leukocytosis, however, persisted despite 10 days of antibiotic therapy. On the 11th day of hospitalization, the patient developed acute chest pain, diaphoresis, and hypotension, prompting an ECG that showed diffuse ST elevations compatible with acute pericarditis. The ensuing echocardiogram showed a new, small circumferential pericardial effusion. The patient was subsequently started on anti-inflammatory medications as well as colchicine for pericarditis. He was then transferred to our tertiary center for possible pericardiocentesis.
A repeat echocardiogram was significant for an evolving pericardial effusion, which now had septations and echo-dense regions that appeared to be complex in nature. The anterior part of the aortic root appeared thickened; however, the image quality was suboptimal (Videos 1-2). Repeat TEE was significant for a thickened aortic root, along the posterior, medial, and anterior aspects, but once again failed to identify a vegetation on the aortic valve cusps (Video 3). Moreover, more echo-dense material was noted within the pericardial space, along the right atrium and right ventricle, than was appreciated on the surface echocardiogram (Video 4).
Video 1
Video 2
Video 3
Video 4
Considering that the initial TEE was not confirmatory for IE nor for aortic root abscess, what would have been the best approach to rule out an infection of the aortic root/annulus?
Show Answer
The correct answer is: C. 18F-FDG PET/CT
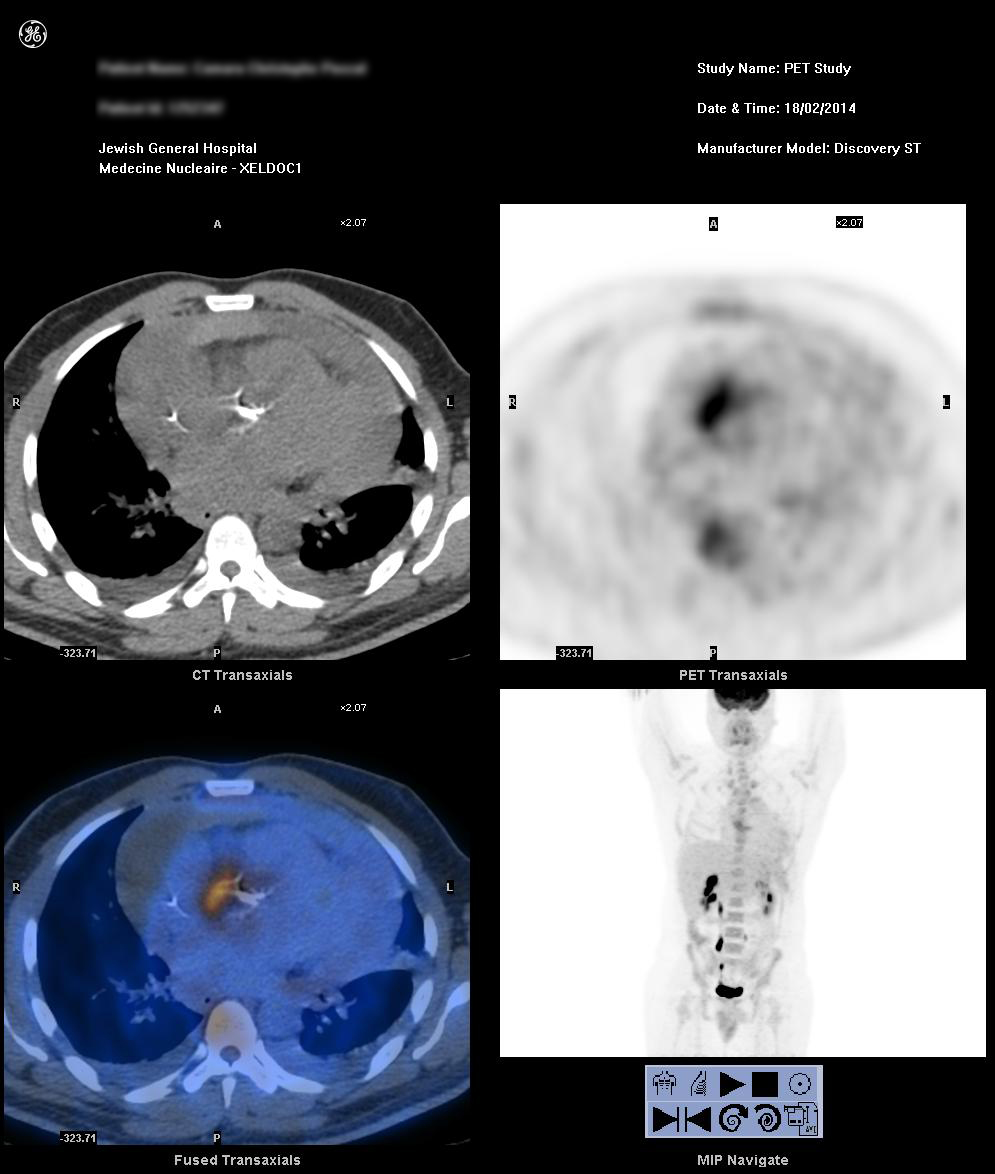
After discussion with the heart team, we opted for a nuclear imaging test to determine if there was an aortic root abscess. An emergency fludeoxyglucose F 18 (18F-FDG) positron emission tomography/computed tomography (PET/CT) elucidated a focus of intense 18F-FDG uptake adjacent to the aortic root calcifications with an extension of the inflammation to the right anterior aspect of the aortic root. These findings were consistent with focal aortitis. Also noted was a pericardial effusion with mixed density encapsulated by a rim of mild 18F-FDG uptake, representing a proteinaceous/hemorrhagic component to the effusion and ongoing pericarditis (Figure 1).
Figure 1
Our patient was subsequently diagnosed with acute aortic valve endocarditis on a native aortic valve that was complicated by both an aortic root abscess and a contained aortic root rupture, leading to hemorrhagic pericarditis. The anteriorly located abscess, retrospectively, was shadowed by the heavily calcified aortic valve on the TEE.
The patient was sent urgently to the operating room where the surgeons noted a tense pericardium with the presence of blood, hemopericardium, and lots of blood clots over the anterior aspect of the right ventricle. They also identified hemorrhagic pericarditis and an infected aortic root especially over the right coronary sinus and the non-coronary sinus. Although the outer aspect of the aortic root did not have frank pus, they identified an area of contained rupture and a walled-off abscess. Finally, the aortic valve was found to be heavily calcified by what was most likely rheumatic disease, upon which vegetations were identified.
The presence of perivalvular extensions of IE is associated with a poor prognosis. These complications include abscess formation, pseudoaneurysm, and fistulae.1 Given that the presence of an aortic root abscess is an urgent indication for surgery, its prompt and accurate diagnosis is mandatory in an attempt to reduce perioperative morbidity and mortality.2
TEE, with its improved image quality and close proximity to the various structures in question along with higher frequency probes, allows for more detailed spatial and temporal resolution to detect a valvar vegetation and any associated complications.3 Moreover, TEE, with a sensitivity of 90%, is felt to be the superior diagnostic imaging modality when compared with TTE (sensitivity of about 50%) when diagnosing abscesses in complicated aortic valve endocarditis.4,5 As such, the European Society of Cardiology (ESC) recommends a TEE if the TTE is of suboptimal quality, if there is a prosthetic valve, or if there is any suspicion of a complication caused by this infectious process.
Anterior aortic root abscesses have classically been more difficult to diagnose. It is more visible in the longitudinal plane and requires multiplane imaging to identify its presence.2 Moreover, the presence of calcifications impedes the transmission of the ultrasound waves on TEE and is an obvious limitation when assessing a calcified aortic valve.6 Consequentially, in our case, the use of alternative imaging was sought to clarify the diagnosis of suspected infected endocarditis.
In the previous iteration of the ESC guidelines for the diagnosis and treatment of endocarditis, a repeat TEE was recommended within 7-10 days of presentation when initial imaging is negative but clinical suspicion of IE remains high.1,7-10 Recent studies, however, have shown the incremental diagnostic value of PET/CT in infections involving heart valve prostheses and devices, when the diagnosis is often difficult. For prosthetic valve endocarditis, Saby et al. found that PET/CT had a sensitivity of 73% and a specificity of 80%. When PET/CT results were combined with the traditional Duke's criteria, the sensitivity and specificity increased from 70 to 97% and from 52 to 91%, respectively, for the diagnosis of IE.1,10 Moreover, the inclusion of PET/CT to the modified Duke's criteria allowed for an earlier diagnosis especially when echocardiography was normal or doubtful and, more importantly, before any infectious damage or adverse event had occurred.10 As such, the latest iteration of the ESC guidelines for the diagnosis and treatment of endocarditis incorporated 18F-FDG PET/CT when faced with diagnostic uncertainty. We, as a team, extrapolated from these data that in the face of heavy calcification, PET/CT would allow us to confirm our suspicion in a case of native valve endocarditis.
Conclusion
TEE, especially in cases of mitral valve endocarditis, is clearly superior to TTE for the diagnosis and evaluation of IE and its associated complications. Aortic valve endocarditis, on the other hand, can sometimes prove to be a diagnostic challenge, especially when evaluating the anterior aortic root for the presence of an abscess. In such circumstances, the TTE and TEE play a complementary role to make a definitive diagnosis. This diagnostic challenge can be accentuated, as shown in this case, by the presence of a prosthesis or heavy calcification. In these circumstances, alternative imaging should be obtained. PET-CT may allow for an earlier definitive diagnosis and avoid progression to serious complications when periaortic abscesses are suspected.
References
Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015;36:3075-128.
Leung DY, Cranney GB, Hopkins AP, Walsh WF. Role of transoesophageal echocardiography in the diagnosis and management of aortic root abscess. Br Heart J 1994;72:175-81.
Karalis DG, Bansal RC, Hauck AJ, et al. Transesophageal echocardiographic recognition of subaortic complications in aortic valve endocarditis. Clinical and surgical implications. Circulation 1992;86:353-62.
Habib G, Badano L, Tribouilloy C, et al. Recommendations for the practice of echocardiography in infective endocarditis. Eur J Echocardiogr 2010;11:202-19.
Daniel WG, Mügge A, Martin RP, et al. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med 1991;324:795-800.
Iung B, Rouzet F, Brochet E, Duval X. Cardiac Imaging of Infective Endocarditis, Echo and Beyond. Curr Infect Dis Rep 2017;19:8.
Habib G, Hoen B, Tornos P, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J 2009;30:2369-413.
Pérez-Vázquez A, Fariñas MC, García-Palomo JD, Bernal JM, Revuelta JM, González-Macías J. Evaluation of the Duke criteria in 93 episodes of prosthetic valve endocarditis: could sensitivity be improved? Arch Intern Med 2000;160:1185-91.
Roque A, Pizzi MN, Cuéllar-Calàbria H, Aguadé-Bruix S. 18F-FDG-PET/CT Angiography for the Diagnosis of Infective Endocarditis. Curr Cardiol Rep 2017;19:15.
Saby L, Laas O, Habib G, et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J Am Coll Cardiol 2013;61:2374-82.