An 88-year-old woman is brought to the emergency department by her family for four hours of epigastric pressure, nausea, and dizziness. She has a past medical history of diabetes and hypertension, well-controlled by metformin and lisinopril, respectively. She lives independently and performs her own activities of daily living. She has had no recent hospitalizations and the past medical history is non-contributory. The patient repeats that she has indigestion and needs something for her stomach.
On physical examination, she is diaphoretic and mildly agitated. Her BP is 100/78 mm Hg in both arms, and the heart rate is regular at 105 bpm. Respiratory rate is 20 breaths per minute. Her weight is 120 lbs. The arterial oxygen saturation is 94% on 4 liters of O2/min administered by nasal cannula. She has jugular venous distention to 8 cm, carotid pulses are brisk, there are bi-basilar rales, and the apex impulse is sustained but not displaced. An S4 is present. Peripheral pulses are symmetric.
Laboratory data: the hemogram is unremarkable, electrolytes are normal, BUN and creatinine are within normal limits, blood glucose is 105 mg/dl and the troponin is 0.28 ng/ml.
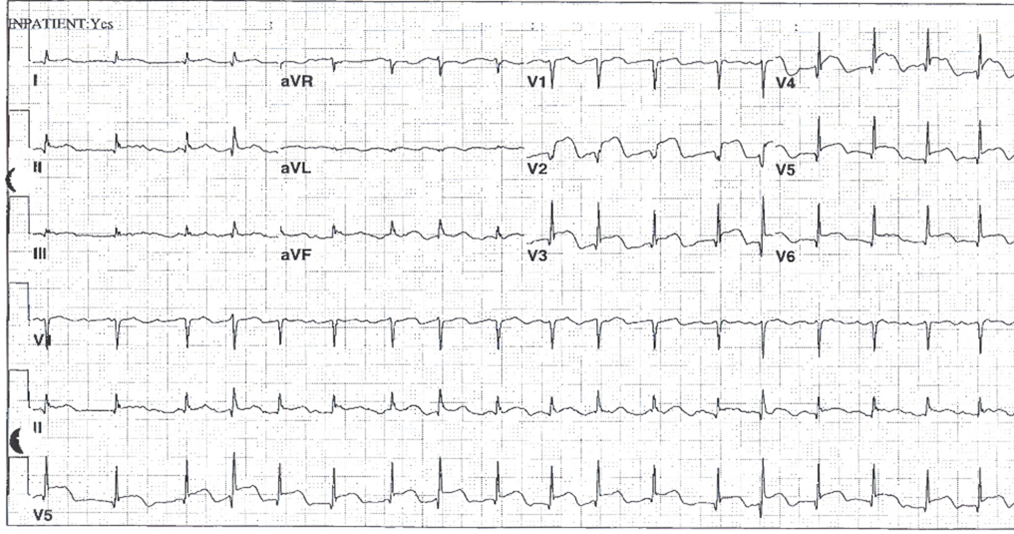
The electrocardiogram is as shown in Figure 1.
Figure 1: Admission EKG
Which of the following is the most likely diagnosis?
Show Answer
The correct answer is: C. Acute ST Elevation Myocardial Infarction (STEMI).
Answer choice A is incorrect because despite the fact that the patient reports indigestion and her symptom complex includes epigastric pressure and nausea, gastrointestinal symptoms, even in the absence of chest pain, are common presentations of acute myocardial infarction at elderly age. Also note that the patient has no prior history of gastrointestinal problems.
Answer choice B is incorrect because although the patient has diabetes, it has been well-controlled and she has no complications of type 2 diabetes mellitus. There were no antecedent symptoms suggestive of gastroparesis.
Answer choice C is correct as older patients, particularly older women, often present with non-chest pain ischemic symptoms and her "GI symptoms" represent myocardial ischemia. The electrocardiogram is characteristic for ST elevation myocardial infarction with marked ST elevation in leads V2-V6.
Answer choice D is incorrect because the patient does not have a pain syndrome compatible with acute pericarditis (no symptoms increased with respiration, no relief on leaning forward), nor does she have any precipitating prodrome. The electrocardiogram shows focal ST elevation compatible with acute myocardial ischemia, rather than the diffuse ST elevation characteristic of acute pericarditis. Further, there is no PR segment displacement of acute pericarditis.
Answer choice E is incorrect. Typically the presentation of aortic dissection, even at elderly age, is severe and sudden onset pain, typically in the back but at times in the chest and arms. Also note that peripheral pulses are intact and the BP is symmetrical in both arms.
Bueno H, Betriu A, Heras M, et al. Primary angioplasty vs. fibrinolysis in very old patients with acute myocardial infarction: TRIANA (TRatamiento del Infarto Agudo de miocardio eN Ancianos) randomized trial and pooled analysis with previous studies. Eur Heart J 2011;32:51-60.
O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;61;485-510.
Alexander KP, Newby LK, Armstrong PW, et al. Acute coronary care in the elderly, part II: ST-segment-elevation myocardial infarction: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: In collaboration with the Society of Geriatric Cardiology. Circulation 2007;115:2570-89.
Saunderson CE, Brogan RA, Simms AD, Sutton G, Batin PD, Gale CP. Acute coronary syndrome management in older adults: guidelines, temporal changes and challenges. Age Ageing 2014;43:450-5.
Veerasamy M, Edwards R, Ford G, et al. Acute coronary syndrome among older patients: a review. Cardiol Rev 2015;23:26-32.
Grosmaitre P, Le Vavasseur O, Yachouh E, et al. Significance of atypical symptoms for the diagnosis and management of myocardial infarction in elderly patients admitted to emergency departments. Arch Cardiovasc Dis 2013;106:586-92.
Newell MC, Henry JT, Henry TD, et al. Impact of age on treatment and outcomes in ST-elevation myocardial infarction. Am Heart J 2011;161:664-72.