Poll Results: Use of CT Angiography For the Evaluation of Coronary Anatomy
Quick Takes
- Coronary CT Angiography (CTA) is increasingly recommended as a useful screening test to confirm (or refute) suspected, significant coronary artery disease in stable ischemic heart disease (SIHD), thus limiting unnecessary cost and the risk of invasive coronary angiography.
- While CTA has been compared to invasive coronary angiography (ICA) over years, recent results show that CTA, while not providing exactly equivalent results to ICA, the results appear to be sufficiently comparative to allow CTA to be used as the initial evaluation tool for moderate probability coronary artery disease in SIHD.
Discussion:
This poll question was derived from two recent publications. First, in a retrospective analysis of the ISCHEMIA Trial,1 Initial screening CTAs for patients (N=1728) randomized to revascularization were compared to ICA. The primary CTA screening for significant (50%) left main stenosis with at least one additional coronary artery with a 50% stenosis correlated with ICA in 92.2% of studies. However, there were limits to the correlation; CTA was predictive of the number of diseased vessels in only 54.5% of cases.2
In Another recent study,3 3,561 patients with stable chest pain and intermediate probability of coronary artery disease were randomized to CTA or ICA for diagnostic evaluation. Initial revascularization was low for both groups (<20%). The composite endpoint (CV death, nonfatal myocardial infarction, or nonfatal stroke) at 3.5 years was low for both groups (2.1 and 3.0%) and not significantly different. Procedure related complications related to revascularization were higher in the ICA group which included more revascularization and were 4 times higher than for patients not receiving revascularization. Thus, while major CV outcomes were not different, the extent of revascularization and associated complications were notably higher.
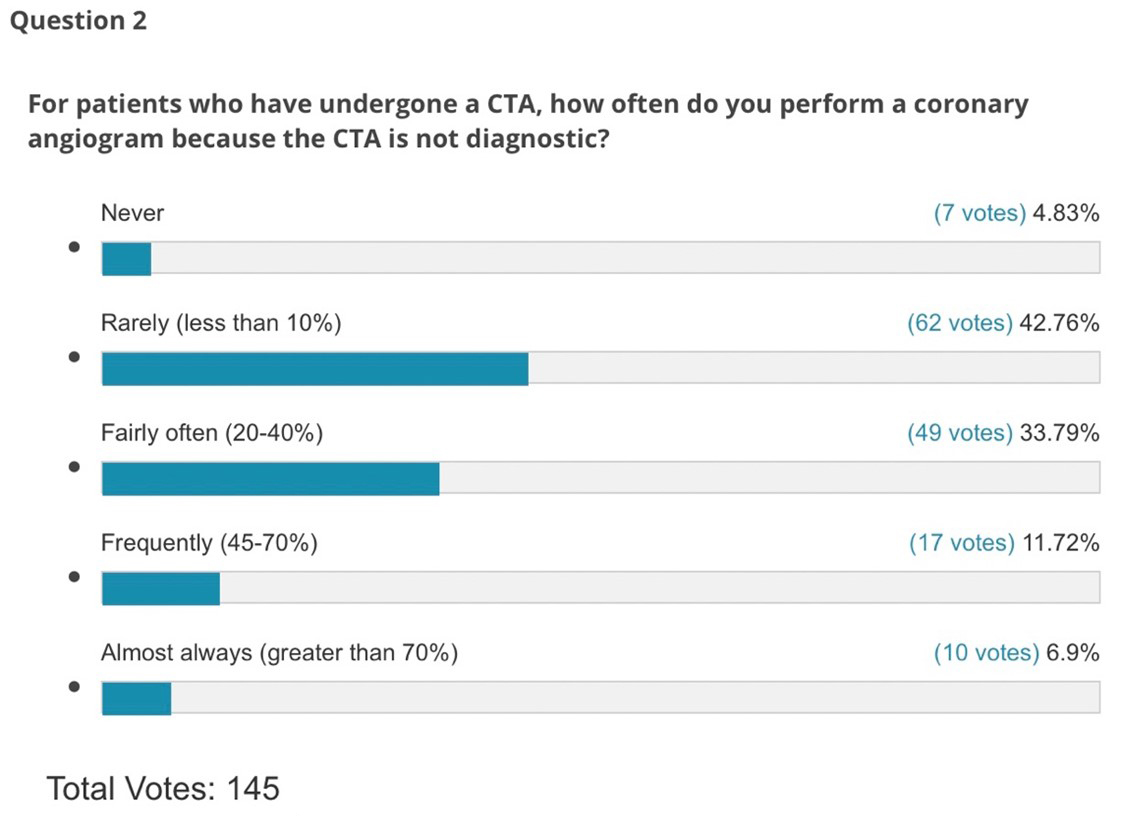
The results of the Poll (Figures 1,2) showed that for Question 1, 28% of respondents never use CTA to screen for presence of and/or extent of coronary artery (Severe left main or multivessel disease), while only 12% of regularly use CTA for screening. Other responses suggested CTA screening in 10, 25 and 50% of cases. Question 2 attempted to address the perceived reliability of the CTA in providing equivalent information to ICA. Interestingly, there was a split in approaches/philosophy with 43% saying they rarely do ICA because the ICA is not diagnostic, while only 18% responded that they do ICA frequently or almost always. My interpretation of these responses is that most accept the results of the CTA in terms of anatomic screening but rarely use CTA as a screening test.
Application of CTA remains challenging in certain circumstances, particularly in patients with heavy calcification or prior stenting, both of which can create artifacts reducing the ability to interpret CTA. Thus, physicians need to assess patients and their CTA results individually to make optimal clinical decisions given that screening ICA based on stress test results demonstrate no significant obstructive disease. Thus, selected properly, CTA has the potential to limit ICA complications. In addition, none of these studies have evaluated the impact of the use of CTFFR technology to enhance the results of CTA and the impact on diagnostic reliability.
Figure 1
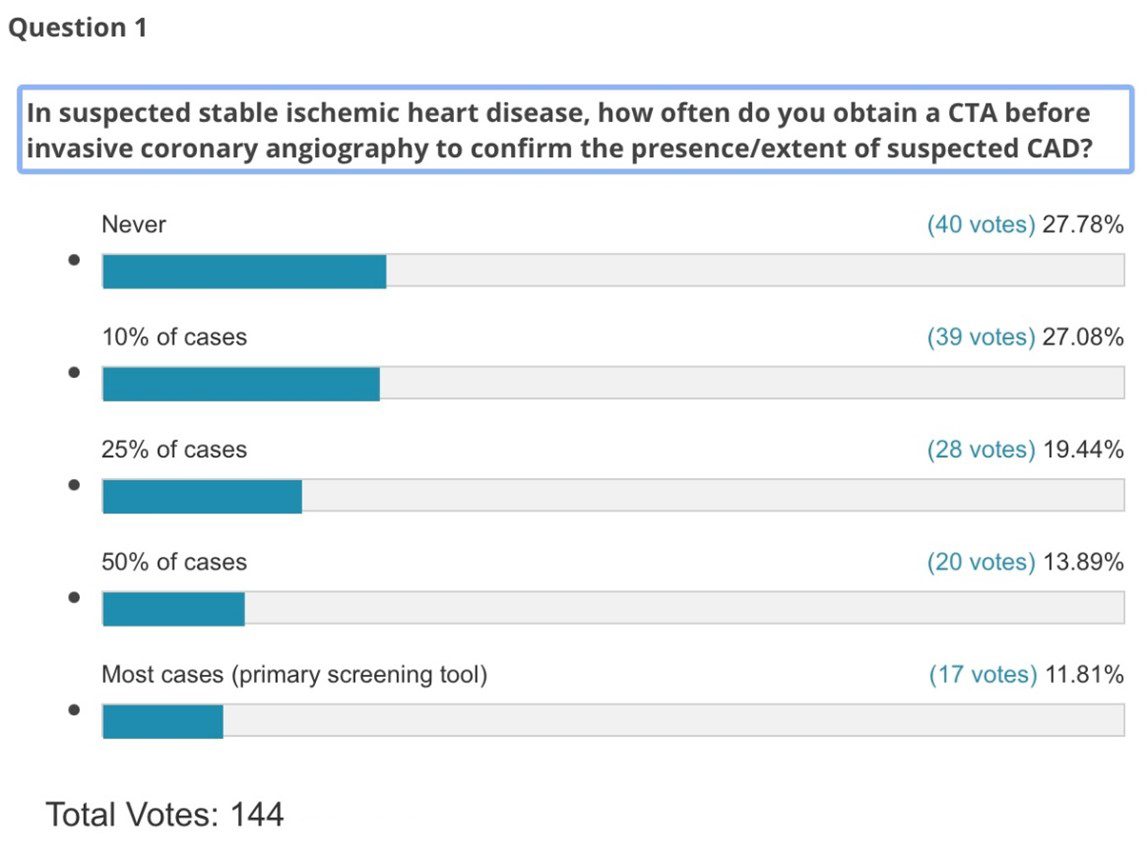
Figure 2
References
- Mancini JGB, Leipsic J, Budoff MJ, et al. Coronary CT angiography followed by invasive angiography in patients with moderate or severe ischemia-insights from the ISCHEMIA trial. JACC Cardiovasc Imag 2021;14: 1384–93.
- Bhatt DL, Benjamin E. Peterson BE. The Emerging Role of Coronary Computed Tomography Angiography in Stable Angina With ISCHEMIA. JACC Cardiovasc Imag 2021;14: 1394-97.
- The DISCHARGE Trial Group. CT or invasive coronary angiography in stable chest pain. N Engl J Med 2022;386:1591- 602.
Clinical Topics: Atherosclerotic Disease (CAD/PAD), Invasive Cardiovascular Angiography and Intervention
Keywords: Coronary Artery Disease, Retrospective Studies, Exercise Test, Reproducibility of Results, Constriction, Pathologic, Myocardial Infarction, Surveys and Questionnaires, Chest Pain, Physicians, Ischemia, Stroke
< Back to Listings