Cutting-Edge Structural Interventions | Hypertrophic Septum: Ablation, Transcatheter Myotomy or Medical Therapy?

Hypertrophic septum affects patients in two ways: it manifests as symptomatic left ventricular outflow (LVOT) obstruction in hypertrophic cardiomyopathy (HCM) or prevents the option for transcatheter mitral valve replacement (TMVR) due to the perceived risk of developing LVOT obstruction.
Surgical myectomy has long been the treatment of choice for achieving septal reduction. However, outcomes vary based on the operator and institutional experience and can be morbid in high surgical risk patients.1
Consequently, there is a growing interest and demand for developing less invasive alternatives. Various transcatheter and medical therapies have been developed and are on the horizon.

Ablation
Alcohol Septal Ablation
First described in 1995,2 alcohol septal ablation is one of the most extensively utilized transcatheter procedures for reducing septal thickness. In this technique, alcohol is purposefully injected into the septal perforator artery supplying the basal septum, inducing intentional infarction and necrosis.
The majority of evidence supporting alcohol septal ablation is derived from the HCM population. Studies indicate effective symptomatic improvement, with approximately 90% achieving NYHA functional class I/II at follow-up, similar to the outcomes of surgical myectomy.3,4
Moreover, alcohol septal ablation demonstrates significantly lower operative mortality (as low as 1.2%) and a minimal risk of iatrogenic ventricular septal defect in the most contemporary era.5
Interventional cardiologists, well-acquainted with alcohol septal ablation technique, now employ it as a bailout option for LVOT obstruction after TMVR6 or as a pre-emptive strategy, effectively enabling TMVR for patients at risk.7
A recognized complication associated with alcohol septal ablation is the disruption of the conduction system, attributed to the Bundle of His located at the basal septum, with 11% requiring in-hospital pacemaker implantation.5 Notably, this risk seems to escalate when employed as a pre-emptive strategy for TMVR, reaching up to 35%.8
Additionally, alcohol septal ablation may not be feasible in cases involving small or mismatched septal perforator arteries, and inadvertent injection or extravasation of alcohol into adjacent arteries can result in an unexpectedly extensive area of infarction.
Radiofrequency Ablation
To address the high morbidity of surgical myectomy and the limitations in anatomical feasibility with alcohol septal ablation, radiofrequency ablation has emerged as a potential alternative.
Several case series have investigated the use of transcatheter endocardial radiofrequency ablation in symptomatic HCM, with most reporting effective reduction in LVOT gradient and symptomatic improvement. The degree of pacemaker implantation varied across studies, ranging from 0 to 21%.9-11
More recently, in a series involving 200 patients, transapical intramyocardial radiofrequency ablation reduced the LVOT gradient from 79.0 (SD 53.0) mm Hg to 14.0 (SD 24.0) mm Hg, with 96% of patients in NYHA functional class I/II at follow-up. At the 30-day mark, major adverse clinical events, including death, emergency surgery and severe effusion requiring intervention, occurred in 10.5%.12
Unsurprisingly, radiofrequency ablation has also been employed before TMVR.13,14 However, though only studied in very small case series, both unipolar and bipolar ablation appear to result in suboptimal gain in the LVOT area, making subsequent TMVR still challenging, and incurring a 100% pacemaker implantation rate.
Transcatheter Myotomy and Myectomy
SESAME
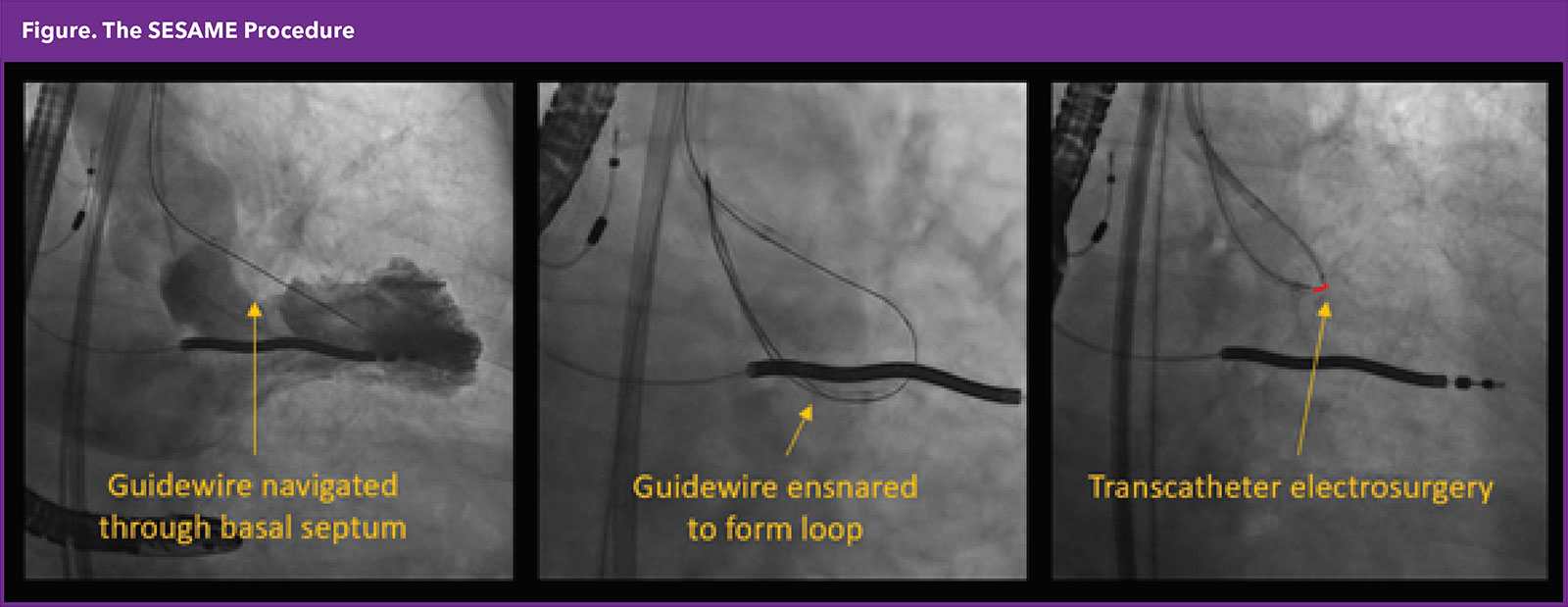
Septal Scoring Along the Midline Endocardium (SESAME) is a technique employing transcatheter electrosurgery to produce a longitudinal splay along the septal bulge, aiming to decrease septal encroachment and relieve or prevent LVOT obstruction.
The procedure involves navigating a stiff guidewire intramyocardially from the basal septum until it reenters the left ventricular cavity, followed by the application of electrosurgery to create the desired splay. This approach is uniquely designed to access the basal septum away from the membranous septum, thus avoiding interference with the conduction system.
The first-in-human application of SESAME has demonstrated its effectiveness in enlarging the LVOT area, enabling successful TMVR without LVOT obstruction.15 Subsequently, there is accumulating experience of its use in HCM, as well as bailout or pre-emptive strategy to facilitate transcatheter procedures, with further investigations currently underway.
Transapical Septal Myectomy
Recently, a group from China reported their experience with the first-in-human transapical beating-heart septal myectomy in 47 patients with drug-refractory symptomatic HCM.16 The investigators introduced a device comprising a resection tube with blades, which was inserted at the basal septum through a minithoracotomy.
The procedural success, defined as achieving a resting/provoked LVOT gradient <30/50 mm Hg and residual mitral regurgitation ≤1+ at three months, was observed in 91%, accompanied by a significant improvement in reported symptoms.
Conduction disturbance was relatively common, with 38.3% developing a left bundle branch block, yet only 2.1% necessitated permanent pacemaker implantation. Other noteworthy complications comprised iatrogenic ventricular septal perforation and left ventricular apical tear, each occurring in 2.1%.
Medical Therapy
Learn More at ACC.24
Start planning now to attend ACC.24, being held from April 6 to 8 in Atlanta, to keep the learning going.
Click here for the Online Planner and the Valvular Heart Disease Learning Pathway. Don't miss sessions including Stretched to the Limit: Bicuspid and Aneurysm-Associated Aortic Valve (Disease #728) and April Adventure: Vexing Vessels (#501).
Visit ACCScientificSession.ACC.org to register today.
In addition to conventional negative inotropic agents (beta-blockers, verapamil and disopyramide), a new class of medical therapy for symptomatic HCM is also emerging – the myosin inhibitors. They work by inhibiting cardiac myosin ATPase, thereby diminishing myosin-actin crossbridge formation and reducing myocardial contractility.
In a randomized trial involving 251 patients with symptomatic HCM, mavacamten demonstrated significantly improved LVOT obstruction, exercise capacity and NYHA functional class compared to placebo at 30 weeks.17
Furthermore, in another study with 112 patients meeting the guideline criteria for septal reduction therapy, only 17.9% continued to meet the criteria after 16 weeks – an outcome significantly different from the placebo group (76.8%).18 A caveat to remember is its potential to reduce LV ejection fraction.
What is the Best Approach?
There is no definitive answer. Management of symptomatic LVOT obstruction in HCM is an evolving field. Currently, there are no randomized trials comparing various septal reduction therapies (such as surgical myectomy, alcohol septal ablation and the series of aforementioned transcatheter septal reduction therapies), nor comparing the new class of medical therapy with septal reduction therapy.
It is an exciting time with a rapid expansion of treatment options. We should be familiar with the pros and cons of each tool and tailor our treatment to the specific needs of the patient in front of us.


This article was authored by Hiroki Ueyama, MD, and Isida Byku, MD, FACC, from the Division of Cardiology, Emory Structural Heart and Valve Center, Emory University Hospital Midtown, in Atlanta, GA.
References
- Mentias A, Smedira NG, Krishnaswamy A, et al. Survival after septal reduction in patients >65 Years old with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol 2023;81:105-15.
- Sigwart U. Non-surgical myocardial reduction for hypertrophic obstructive cardiomyopathy. Lancet 1995;346:211-4.
- Liebregts M, Faber L, Jensen MK, et al. Outcomes of alcohol septal ablation in younger patients with obstructive hypertrophic cardiomyopathy. JACC Cardiovasc Interv 2017;10:1134-43.
- Kimmelstiel C, Zisa DC, Kuttab JS, et al. Guideline-based referral for septal reduction therapy in obstructive hypertrophic cardiomyopathy is associated with excellent clinical outcomes. Circ Cardiovasc Interv 2019;12:e007673.
- Altibi AM, Ghanem F, Zhao Y, et al. Hospital procedural volume and clinical outcomes following septal reduction therapy in obstructive hypertrophic cardiomyopathy. J Am Heart Assoc 2023;12:e028693.
- Guerrero M, Wang DD, Himbert D, et al. Short-term results of alcohol septal ablation as a bail-out strategy to treat severe left ventricular outflow tract obstruction after transcatheter mitral valve replacement in patients with severe mitral annular calcification. Catheter Cardiovasc Interv 2017;90:1220-6.
- Wang DD, Guerrero M, Eng MH, et al. Alcohol septal ablation to prevent left ventricular outflow tract obstruction during transcatheter mitral valve replacement: First-in-man study. JACC Cardiovasc Interv 2019;12:1268-79.
- Elhadi M, Guerrero M, Collins JD,et al. Safety and outcomes of alcohol septal ablation prior to transcatheter mitral valve replacement. J Soc Cardiovasc Angiography Interv 2022;100396.01.09.2022.
- Lawrenz T, Borchert B, Leuner C, et al. Endocardial radiofrequency ablation for hypertrophic obstructive cardiomyopathy: acute results and 6 months' follow-up in 19 patients. J Am Coll Cardiol 2011;57:572-6.
- Kong L, Zhao Y, Pan H, et al. A modified endocardial radiofrequency ablation approach for hypertrophic obstructive cardiomyopathy guided by transthoracic echocardiography: a case series. Ann Transl Med 2021;9:1006.
- Crossen K, Jones M, Erikson C. Radiofrequency septal reduction in symptomatic hypertrophic obstructive cardiomyopathy. Heart Rhythm 2016;13:1885-90.
- Zhou M, Ta S, Hahn RT, et al. Percutaneous Intramyocardial septal radiofrequency ablation in patients with drug-refractory hypertrophic obstructive cardiomyopathy. JAMA Cardiol 2022;7:529-38.
- Killu AM, Collins JD, Eleid MF, et al. Preemptive septal radiofrequency ablation to prevent left ventricular outflow tract obstruction with transcatheter mitral valve replacement: A case series. Circ Cardiovasc Interv 2022;15:e012228.
- Hoskins MH, Lisko JC, Greenbaum AB, et al. Septal bipolar ablation to prevent left ventricular outflow tract obstruction after transcatheter mitral valve implantation. Circ Cardiovasc Interv 2023;16:e013333.
- Greenbaum AB, Khan JM, Bruce CG, et al. Transcatheter myotomy to treat hypertrophic cardiomyopathy and enable transcatheter mitral valve replacement: First-in-human report of septal scoring along the midline endocardium. Circ Cardiovasc Interv 2022;15:e012106.
- Fang J, Liu Y, Zhu Y, et al. First-in-human transapical beating-heart septal myectomy in patients with hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol 2023;82:575-86.
- Olivotto I, Oreziak A, Barriales-Villa R, et al. Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2020;396:759-69.
- Desai MY, Owens A, Geske JB, et al. Myosin inhibition in patients with obstructive hypertrophic cardiomyopathy referred for septal reduction therapy. J Am Coll Cardiol 2022;80:95-108.
Clinical Topics: Arrhythmias and Clinical EP, Cardiac Surgery, Congenital Heart Disease and Pediatric Cardiology, Heart Failure and Cardiomyopathies, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Aortic Surgery, Cardiac Surgery and Arrhythmias, Cardiac Surgery and CHD and Pediatrics, Cardiac Surgery and Heart Failure, Congenital Heart Disease, CHD and Pediatrics and Arrhythmias
Keywords: Cardiology Magazine, ACC Publications, Ablation Techniques, Heart Septal Defects, Ventricular, Electrosurgery, Cardiomyopathy, Hypertrophic, Hypertrophic Cardiomyopathy, Ventricular Outflow Obstruction