Cover Story | Renal Denervation: From Controversy to Comeback in Hypertension Care

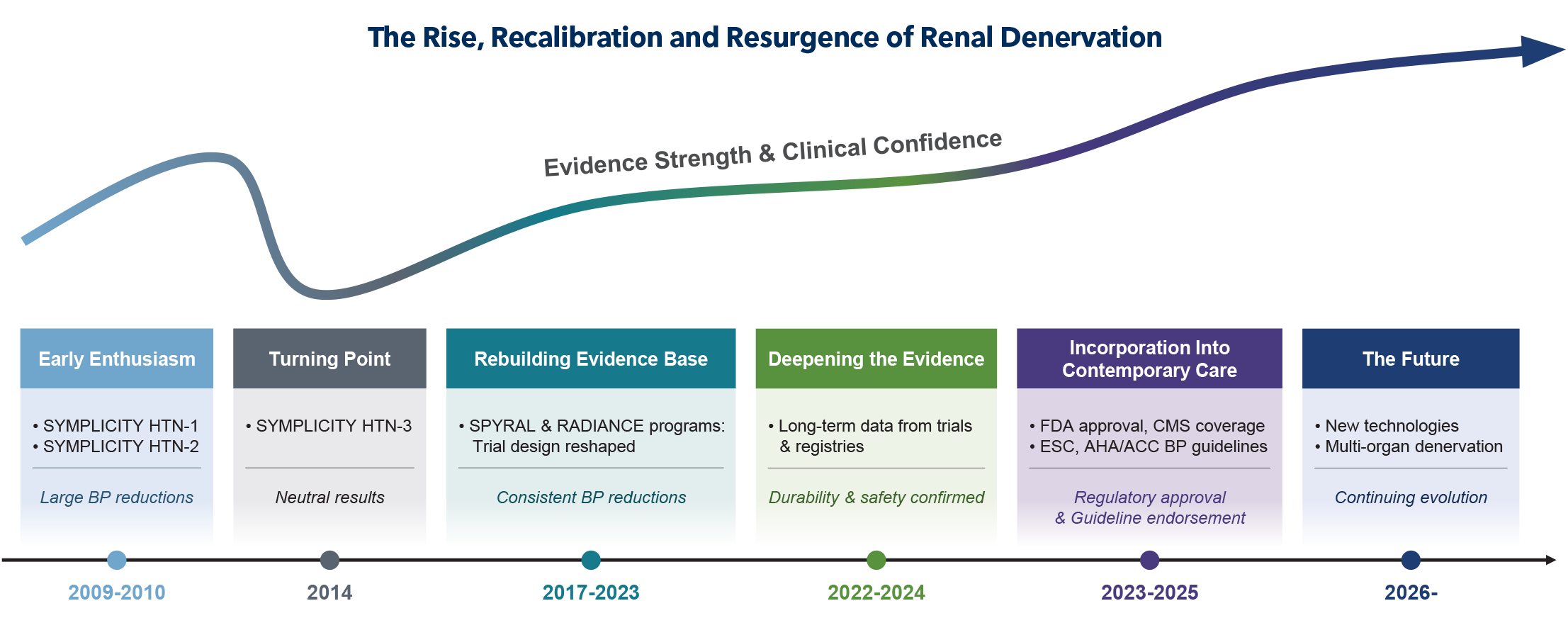
Few therapies in cardiovascular medicine have traveled a path as turbulent as renal denervation. Once hailed as a breakthrough for uncontrolled hypertension, the field was abruptly shaken by neutral findings from SYMPLICITY HTN-3. What followed was not the end of the story – but a recalibration. A decade later, renal denervation has re-emerged with stronger evidence, refined technique and renewed clinical relevance.
The Early Enthusiasm Around Renal Denervation
The advent of a percutaneous approach to "denervate" the renal sympathetic system initially sparked broad enthusiasm. The appeal was intuitive – interrupt renal sympathetic signaling, and blood pressure (BP) would fall. Early prospective studies appeared to meet this expectation, reporting striking reductions in BP.
In the first-in-human proof-of-principle study, SYMPLICITY HTN-1, office systolic BP (SBP) decreased by 14 mm Hg at one month after radiofrequency-based renal denervation, with the reduction reaching 27 mm Hg at 12 months.1 The subsequent randomized trial, SYMPLICITY HTN-2, demonstrated an even more dramatic effect at six months, with a 32 mm Hg reduction in office SBP in the denervation group vs. no change in the control group (medical therapy alone).2
A Turning Point: Lessons From SYMPLICITY HTN-3
Following early enthusiasm, renal denervation entered a period of critical reassessment, with investigators aiming to distinguish potential placebo effects from the true physiologic impact of the procedure.
SYMPLICITY HTN-3, the first sham-controlled randomized clinical trial evaluating radiofrequency-based renal denervation, enrolled 535 patients with uncontrolled hypertension across 88 sites in the U.S.3 At six months, office SBP fell by 14.1 mm Hg in the denervation group – but also by an unexpectedly large 11.7 mm Hg in the sham-control group. As a result, the trial did not meet the prespecified 5 mm Hg superiority margin of renal denervation over the sham procedure. This neutral finding tempered the field's early enthusiasm for percutaneous modulation of the renal sympathetic system.
However, subsequent reviews of the trial's design and conduct identified several important limitations, providing critical lessons for future evaluation of the device. Changes in background antihypertensive medications before the primary endpoint assessment occurred in up to 40% of participants, confounding the randomized comparison. Ablation was limited to the main renal arteries, despite emerging evidence of high sympathetic nerve density in distal branches and accessory arteries. Office BP – less precise and reliable than ambulatory measurements – was used as the primary endpoint measure. Finally, the older-generation single-electrode catheter could not ensure uniform ablation of renal arteries.
Rebuilding the Evidence Base With Next-Generation Trials
The lessons learned from SYMPLICITY HTN-3 led to a fundamental reshaping of subsequent trial design. Background antihypertensive medications were more strictly controlled, and trials were conducted separately in off-medication and on-medication cohorts. The procedure became more standardized, with greater emphasis on complete ablation extending to distal branches and accessory arteries. Ambulatory BP replaced office measurements as the primary endpoint. Meanwhile, iterative advances in catheter technology enabled more uniform and circumferential energy delivery.
What followed was renewed confidence in the efficacy of renal denervation – this time supported by more rigorous evidence. In the SPYRAL trial program evaluating the radiofrequency-based Symplicity Spyral system (Medtronic), sham-adjusted reductions in 24-hour ambulatory SBP were consistently observed across both off- and on-medication cohorts: 5.0 mm Hg at three months in OFF MED pilot trial,4 3.9 mm Hg at three months in OFF MED pivotal trial,5 and 7.4 mm Hg at six months in ON MED pilot trial.6 Similar reductions were also reported with other radiofrequency-based renal denervation systems.7,8
The evidence was also extended beyond the radiofrequency-based systems to include the ultrasound-based Paradise system (ReCor Medical). In the off-medication RADIANCE-HTN SOLO and RADIANCE II trials, sham-adjusted reductions in daytime ambulatory SBP reached 6.3 mm Hg at two months,9,10 while RADIANCE-HTN TRIO demonstrated a 4.5 mm Hg reduction at two months in an on-medication cohort.11
Deepening the Evidence: Durability and Safety
As the evidence base for renal denervation matured, attention shifted from short-term efficacy to questions of durability. The accumulating data from randomized trials and real-world registries offered a reassuring answer: BP reductions were maintained, and in most cases amplified, over longer follow-up.
For instance, in SYMPLICITY HTN-3, the sham-adjusted reduction in office SBP reached 22.1 mm Hg at three years;12 in SPYRAL HTN-ON MED, reductions in 24-hour ambulatory SBP were 10.0 mm Hg at 36 months in the pilot cohort13 and 5.7 mm Hg at 24 months in the full cohort14 – each exceeding the magnitude observed at six months. BP reductions were also sustained through 36 months in RADIANCE-HTN SOLO and RADIANCE-HTN TRIO.15,16
Real-world registries echoed these findings: BP declined most steeply within the first three to six months, then continued to fall more gradually over time – an effect that, in some cohorts, has extended to nearly a decade.17,18
Renal denervation has also demonstrated a favorable safety profile. The incidence of adverse events – including vascular complications, renal artery stenosis, hypertensive crisis or emergency, stroke and all-cause death – was generally less than 1% through primary endpoint assessment,19 with no additional safety concerns emerging during longer-term follow-up.17,20
Incorporation Into Contemporary Hypertension Care
Based on the totality of the evidence, the U.S. Food and Drug Administration (FDA) approved the Paradise (ReCor Medical) and Symplicity Spyral (Medtronic) renal denervation systems in November 2023. This regulatory milestone marked an important inflection point, formally introducing renal denervation into contemporary clinical practice.
Regulatory approval, however, did not immediately translate into widespread adoption. The primary barrier was the absence of insurer reimbursement. Unlike certain device-based therapies that can be performed adjunctively during routine procedures (e.g., intravascular lithotripsy or drug-coated balloons), renal denervation is a standalone intervention and therefore depends on dedicated coverage pathways. The National Coverage Determination (NCD) issued by the U.S. Centers for Medicare & Medicaid Services (CMS) in October 2025 substantially reduced this barrier to real-world adoption. Since then, several private insurers followed with coverage decisions, facilitating more consistent access across health systems.
International guidelines have also endorsed renal denervation as an adjunctive therapy for BP control, with the 2023 European Society of Hypertension, 2024 European Society of Cardiology, and 2025 ACC/AHA BP guidelines providing recommendations for its use in patients with resistant or uncontrolled hypertension.
Beyond the Comeback: The Future of Renal Denervation
Renal denervation continues to evolve, with new systems employing alternative ablative mechanisms now under investigation. An intravascular ultrasound-based system (TIVUS, SoniVie) is currently being tested in a sham-controlled trial, while an alcohol-mediated system (Peregrine, Ablative Solutions) has already demonstrated efficacy in two randomized trials,21,22 with a separate pivotal trial underway (NCT07083765).
A multi-organ denervation approach – targeting both the common hepatic and renal sympathetic systems – is also emerging. Early clinical data suggest that this strategy may yield reductions in both 24-hour ambulatory BP and glycated hemoglobin (HbA1c),23 raising the possibility of broader and more profound cardiometabolic benefits. The ongoing SPYRAL GEMINI Pilot Study (NCT06907147) is further evaluating this approach in both off-medication and on-medication cohorts to better define its efficacy and safety.
Beyond ongoing device innovation, the next phase of evidence generation will increasingly rely on real-world data and prospective registries. Recently, the ACC announced a partnership with Beth Israel Deaconess Medical Center's Smith Center for Outcomes Research to develop a quality registry aimed at evaluating short- and long-term efficacy and safety of renal denervation in a broad, unselected U.S. patient population. Such efforts will be critical to translating trial evidence into everyday practice and further refining the role of renal denervation in contemporary hypertension care.
From Controversy to Clinical Relevance
The story of renal denervation highlights the importance of rigorous evaluation, iterative refinement and persistence in innovation. With durable efficacy, reassuring safety, regulatory approval and guideline incorporation, the therapy has entered a new phase of clinical relevance. As research continues and implementation expands, the focus now turns to defining its optimal role within contemporary hypertension care.

This article was authored by Hyeok-Hee Lee, MD, PhD, research fellow in Advanced Hypertension and Vascular Medicine at Beth Israel Deaconess Medical Center (BIDMC), and Eric A. Secemsky, MD, RPVI, MSc, FACC, director of Vascular Intervention at BIDMC and section head of Interventional Cardiology and Vascular Research at the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology at BIDMC, and associate professor of medicine at Harvard Medical School, all in Boston.
References
- Krum H, Schlaich M, Whitbourn R, et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet. 2009;373(9671):1275-1281. https://doi.org/10.1016/s0140-6736(09)60566-3.
- Esler MD, Krum H, Sobotka PA, et al. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010;376(9756):1903-1909. https://doi.org/10.1016/s0140-6736(10)62039-9.
- Bhatt DL, Kandzari DE, O'Neill WW, et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370(15):1393-1401. https://doi.org/10.1056/NEJMoa1402670.
- Townsend RR, Mahfoud F, Kandzari DE, et al. Catheter-based renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications (SPYRAL HTN-OFF MED): a randomised, sham-controlled, proof-of-concept trial. Lancet. 2017;390(10108):2160-2170. https://doi.org/10.1016/s0140-6736(17)32281-x.
- Böhm M, Kario K, Kandzari DE, et al. Efficacy of catheter-based renal denervation in the absence of antihypertensive medications (SPYRAL HTN-OFF MED Pivotal): a multicentre, randomised, sham-controlled trial. Lancet. 2020;395(10234):1444-1451. https://doi.org/10.1016/s0140-6736(20)30554-7.
- Kandzari DE, Böhm M, Mahfoud F, et al. Effect of renal denervation on blood pressure in the presence of antihypertensive drugs: 6-month efficacy and safety results from the SPYRAL HTN-ON MED proof-of-concept randomised trial. Lancet. 2018;391(10137):2346-2355. https://doi.org/10.1016/s0140-6736(18)30951-6.
- Jiang X, Mahfoud F, Li W, et al. Efficacy and Safety of Catheter-Based Radiofrequency Renal Denervation in Chinese Patients With Uncontrolled Hypertension: The Randomized, Sham-Controlled, Multi-Center Iberis-HTN Trial. Circulation. 2024;150(20):1588-1598. https://doi.org/10.1161/circulationaha.124.069215.
- Li Y, Gao F, Ren C, et al. The Netrod™ six-electrode radiofrequency renal denervation system for uncontrolled hypertension: a sham-controlled trial. Eur Heart J. 2024;45(44):4761-4764. https://doi.org/10.1093/eurheartj/ehae703.
- Azizi M, Schmieder RE, Mahfoud F, et al. Endovascular ultrasound renal denervation to treat hypertension (RADIANCE-HTN SOLO): a multicentre, international, single-blind, randomised, sham-controlled trial. Lancet. 2018;391(10137):2335-2345. https://doi.org/10.1016/s0140-6736(18)31082-1.
- Azizi M, Saxena M, Wang Y, et al. Endovascular Ultrasound Renal Denervation to Treat Hypertension: The RADIANCE II Randomized Clinical Trial. JAMA. 2023;329(8):651-661. https://doi.org/10.1001/jama.2023.0713.
- Azizi M, Sanghvi K, Saxena M, et al. Ultrasound renal denervation for hypertension resistant to a triple medication pill (RADIANCE-HTN TRIO): a randomised, multicentre, single-blind, sham-controlled trial. Lancet. 2021;397(10293):2476-2486. https://doi.org/10.1016/s0140-6736(21)00788-1.
- Bhatt DL, Vaduganathan M, Kandzari DE, et al. Long-term outcomes after catheter-based renal artery denervation for resistant hypertension: final follow-up of the randomised SYMPLICITY HTN-3 Trial. Lancet. 2022;400(10361):1405-1416. https://doi.org/10.1016/s0140-6736(22)01787-1.
- Mahfoud F, Kandzari DE, Kario K, et al. Long-term efficacy and safety of renal denervation in the presence of antihypertensive drugs (SPYRAL HTN-ON MED): a randomised, sham-controlled trial. Lancet. 2022;399(10333):1401-1410. https://doi.org/10.1016/s0140-6736(22)00455-x.
- Kandzari DE, Mahfoud F, Townsend RR, et al. Long-term safety and efficacy of renal denervation: 24-month results from the SPYRAL HTN-ON MED Trial. Circ Cardiovasc Interv. 2025;18(7):e015194. https://doi.org/10.1161/circinterventions.125.015194.
- Rader F, Kirtane AJ, Wang Y, et al. Durability of blood pressure reduction after ultrasound renal denervation: three-year follow-up of the treatment arm of the randomised RADIANCE-HTN SOLO trial. EuroIntervention. 2022;18(8):e677-e685. https://doi.org/10.4244/eij-d-22-00305.
- Bloch MJ, Kirtane AJ, Azizi M, et al. 36-month durability of ultrasound renal denervation for hypertension resistant to combination therapy in RADIANCE-HTN TRIO. Hypertens Res. 2024;47(12):3467-3472. https://doi.org/10.1038/s41440-024-01854-w.
- Mahfoud F, Townsend RR, Kandzari DE, et al. Long-Term, patient-level analysis of radiofrequency renal denervation in the SYMPLICITY Clinical Trial Program. JACC Adv. 2025;4(3):101606. https://doi.org/10.1016/j.jacadv.2025.101606.
- Sesa-Ashton G, Nolde JM, Muente I, et al. Long-term blood pressure reductions following catheter-based renal denervation: A systematic review and meta-analysis. Hypertension. 2024;81(6):e63-e70. https://doi.org/10.1161/hypertensionaha.123.22314.
- Vukadinović D, Lauder L, Kandzari DE, et al. Effects of catheter-based renal denervation in hypertension: A systematic review and meta-analysis. Circulation. 2024;150(20):1599-1611. https://doi.org/10.1161/circulationaha.124.069709.
- Mahfoud F, Mancia G, Schmieder RE, et al. Cardiovascular risk reduction after renal denervation according to time in therapeutic systolic blood pressure range. J Am Coll Cardiol. 2022;80(20):1871-1880. https://doi.org/10.1016/j.jacc.2022.08.802.
- Kandzari DE, Weber MA, Pathak A, et al. Effect of alcohol-mediated renal denervation on blood pressure in the presence of antihypertensive medications: Primary results from the TARGET BP I randomized clinical trial. Circulation. 2024;149(24):1875-1884. https://doi.org/10.1161/circulationaha.124.069291.
- Pathak A, Rudolph UM, Saxena M, et al. Alcohol-mediated renal denervation in patients with hypertension in the absence of antihypertensive medications. EuroIntervention. 2023;19(7):602-611. https://doi.org/10.4244/eij-d-23-00088.
- Sievert K, Gogorishvili I, Sievert H. TCT-208 Multi-Organ Arterial Denervation for the Treatment of Type 2 Diabetes Mellitus and Its Comorbidities (NECTAR IV Trial). J Am Coll Cardiol. 2025;86 (17_Supplement):B93.
Clinical Topics: Prevention, Hypertension
Keywords: Cardiology Magazine, ACC Publications, CM-Apr-2026, Antihypertensive Agents, Blood Pressure, Prospective Studies, Denervation, Hypertension