New Insights on Thoracic Aortic Aneurysms in Marfan Syndrome, Ehlers-Danlos, Loeys-Dietz Syndrome
Two studies published in JACC on June 16 provide new insights on arterial events associated with heritable thoracic aortic disease (TAD) and the relative risk in patients with pathogenic variants (PVs) as well as the prevalence, characteristics and clinical outcomes of arterial aneurysms (AAs) in Loeys-Dietz Syndrome (LDS).
In a study using data from the worldwide Montalcino Aortic Consortium, Ernesto Calderon-Martinez, MD, et al., found significant gene- and sex-specific differences in the prevalence and age of onset of arterial events associated with heritable TAD genes, emphasizing the need for tailored counseling and surveillance based on the causative gene.
In this retrospective cohort study, they sought to define the relative risk of arterial and aortic events in individuals with PVs in the FBN1, COL3A1 and TGF-β pathway genes. The authors note that arterial aneurysms, dissections and ruptures are associated with PVs in COL3A1, which is responsible for vascular Ehlers-Danlos syndrome, but arterial events are rare in Marfan syndrome due to PVs in FBN1 and poorly characterized in [LDS] due to PVs in the transforming growth factor TGF-β pathway genes.
Results showed there were arterial events in 83 individuals within the total cohort of 1,780 individuals with PVs in the COL3A1 gene (n=25), FBN1 gene (n=1,028) and TGF-β pathway genes (TGFBR1, n=137; TGFBR, 2 n=168; SMAD3, n=196; TGFB2, n=126).
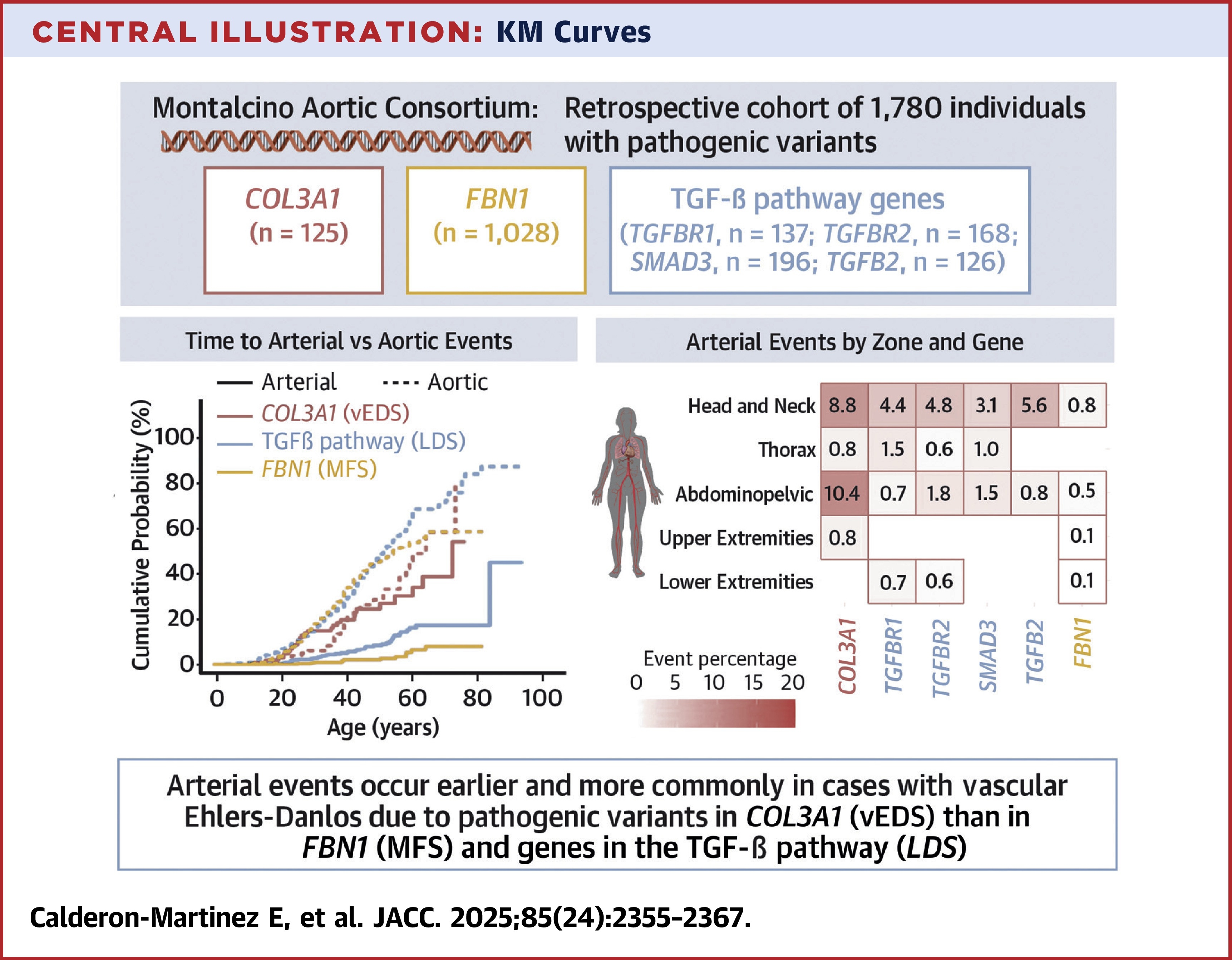
The highest prevalence for events was among patients with COL3A1 (20%), followed by TGFBR2 (8%), TGFBR1 (7%), TGFB2 (6%), SMAD3 (6%) and FBN1 (2%). Researchers found that aortic events were significantly earlier and more penetrant than arterial events for the TGF- β genes and FBN1 but not for COL3A1. Men with COL3A1 had earlier and more arterial events compared with men with TGF-β genes, and these differences were not observed in women. Arterial events in those with the FBN1 PV occur primarily in men.
"Our study underscores the importance of personalized medical care in managing participants with a PV in a gene that predisposes to HTAD, guided by the specific gene and variant type, age and sex of the patient, and their individual risk factors," write the authors.
"The paper is a landmark in the field, due to its size, harmonization of and detailed data collection, and the specificity with which the outcomes are ascertained," write Marion Hofmann Bowman, MD, PhD, and Kim A. Eagle, MD, MACC, in an accompanying editorial comment. "The findings from this study raise hope for building a future risk calculator that incorporates genetic diagnosis, systemic features, and cardiovascular risk factors to further inform optimal and efficient surveillance imaging."
In another retrospective cohort study, Andrew W. Koefoed, BA; Alan C. Braverman, MD, FACC, et al., found that extra-aortic AAs may lead to clinical events including arterial dissection and rupture, thus head to pelvis imaging at diagnosis and follow-up is recommended for patients with LDS.
Their study included 103 patients (53% women) from 60 families with LDS 1 through 5 caused by pathogenic/likely pathogenic variants in TGFBR1, TGFBR2, SMAD3, TGFB2 and TGFB3. The patients were evaluated at Washington University in St. Louis School of Medicine/Barnes-Jewish Hospital between 1998 and 2023 to determine the prevalence, characteristics and clinical outcomes of AAs in LDS. Clinical information, imaging data and outcomes related to AAs were compiled.
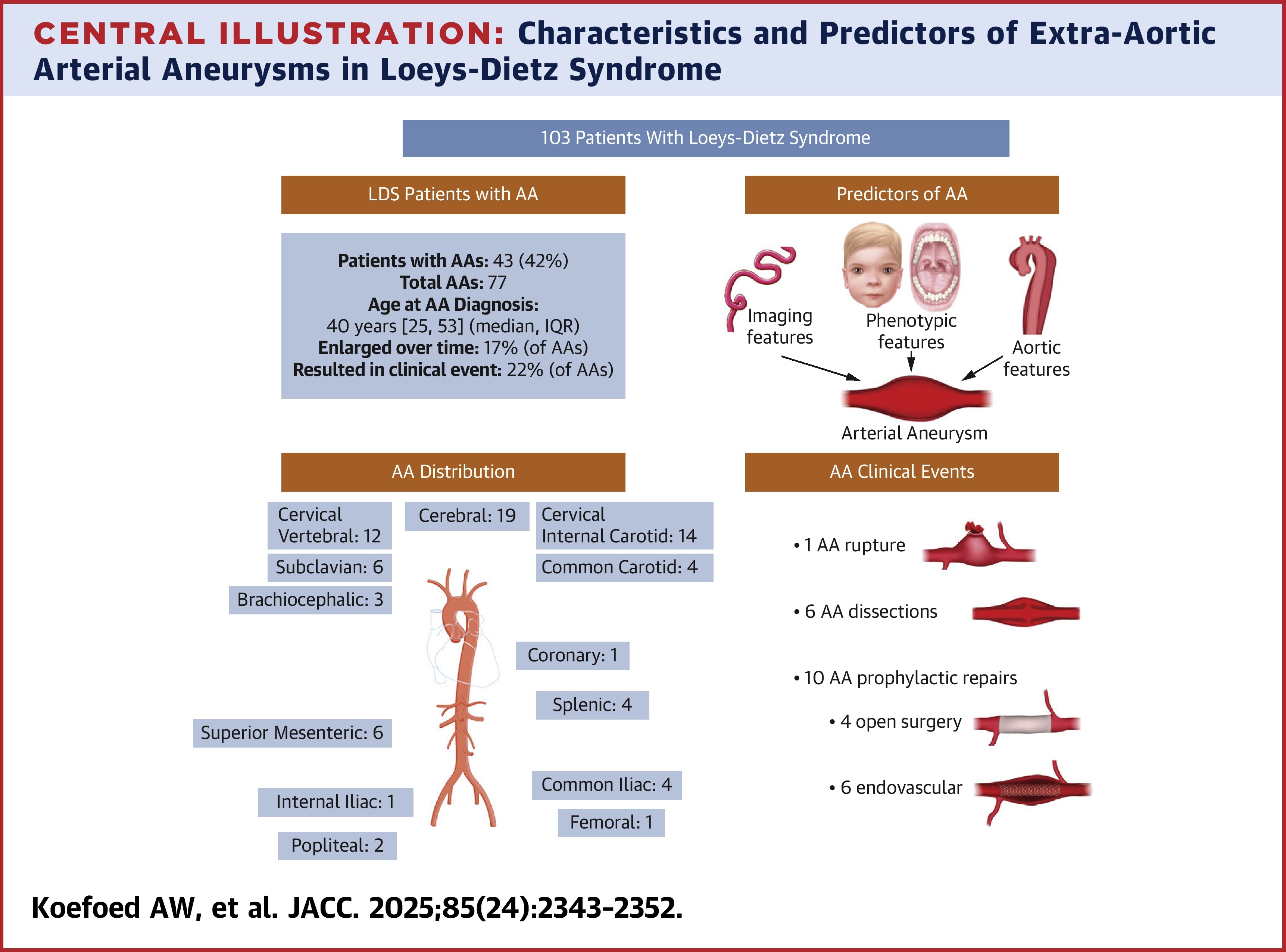
Researchers identified 77 AAs in 43 patients (17 AAs in nine patients with TGFBR1 variants, 33 AAs in 15 patients with TGFBR2, 15 AAs in eight patients with SMAD3, nine AAs in eight patients with TGFB2 and three AAs in three patients with TGFB3). Additionally, 75% of AAs were in the arch vessels or cerebral circulation. The median age of participants was 44 years, median follow-up was six years and the median age at AA diagnosis was 40 years.
"Our data demonstrate that AAs are common in LDS, present in 42% of our cohort, and are present in all five LDS genotypes," write the authors. "AAs most commonly involve the arch vessels and cerebral circulation but occur throughout the entire arterial tree." They note that AAs occur at similar rates in men and women, occur throughout the lifespan and may be diagnosed when LDS is diagnosed or may develop years later."
"…these findings highlight the importance of regular surveillance imaging of AAs and suggest that AAs may be a marker of increased risk of aortic complications," writes Umberto Campia, MD, FACC, in an accompanying editorial comment. "In summary, this study builds a foundation for refining how we follow patients with LDS, not just based on genotype, but also on evolving imaging patterns."
Citations:
- Calderon-Martinez E, Velasco W, Guo, D. et al. Differences in Arterial Events in Vascular Ehlers-Danlos, Loeys-Dietz, and Marfan Syndrome. JACC. Published online June 16, 2025. 85 (24) 2355–2367. doi: 10.1016/j.jacc.2025.04.023
- Koefoed A, Huguenard A, Johnson G, et al. Characterization of Arterial Aneurysms in Loeys-Dietz Syndrome. JACC. Published online June 16, 2025. 85 (24) 2343–2352. doi: 10.1016/j.jacc.2025.04.020
Clinical Topics: Cardiac Surgery, Congenital Heart Disease and Pediatric Cardiology, Vascular Medicine, Aortic Surgery, Cardiac Surgery and CHD and Pediatrics, Congenital Heart Disease
Keywords: Loeys-Dietz Syndrome, Marfan Syndrome, Ehlers-Danlos Syndrome, Thoracic Diseases, Aortic Aneurysm, Thoracic
< Back to Listings