CMR: Component of Value and Quality
With the supervision of the ACC Imaging Section Writing Group editors, Fawaz Alenezi, MD, and Ahmed Sami Abuzaid, MBBS, FACC, will publish a periodic, multipart series of articles related to the utility of cardiac magnetic resonance (CMR) imaging in cardiovascular disease. In this first article, we highlight the component of value and quality of CMR.
Over the history of cardiovascular imaging, a multitude of techniques have been used to study cardiac structure and function (echocardiography, cardiac computed tomography, nuclear imaging and CMR). No single imaging modality is unique for assessment of cardiac structure and function, and a variety of imaging modalities may be used to diagnose and identify patients at risk for cardiovascular disease. However, each test has unique limitations. Surprisingly, the choice of imaging modality sometimes comes down to local availability, cost or expertise, instead of the technique best suited for a given patient or disease. CMR has the advantage of being both flexible and adaptable for functional and anatomical assessment of a wide range of cardiovascular disease. It can generate images akin to echocardiography (cines, flow), while providing high spatial resolution (similar to computed tomography). Other advantages are high tissue contrast, lack of radiation, the ability to assess myocardial perfusion with stress testing, and the depiction of both viable and non-viable myocardium using delayed-enhancement MRI (DE-MRI). DE-MRI has been validated against pathology and used as an endpoint in various multi-center clinical trials. Furthermore, CMR provides an unconstrained field of view, regardless of the patient's body habitus.
These advantages often make CMR the modality of choice in myocardial ischemia, viability and congenital heart disease. Some have considered it a "one-stop-shop" in the assessment of cardiovascular disease. Currently, CMR is the noninvasive gold standard method for left and right ventricular volumes assessment. In addition, CMR is a valuable tool for the evaluation of patients with nonischemic cardiomyopathy (cardiac amyloidosis, hypertrophic cardiomyopathy, arrhythmogenic right ventricular dysplasia and cardiac sarcoidosis) and myocarditis.
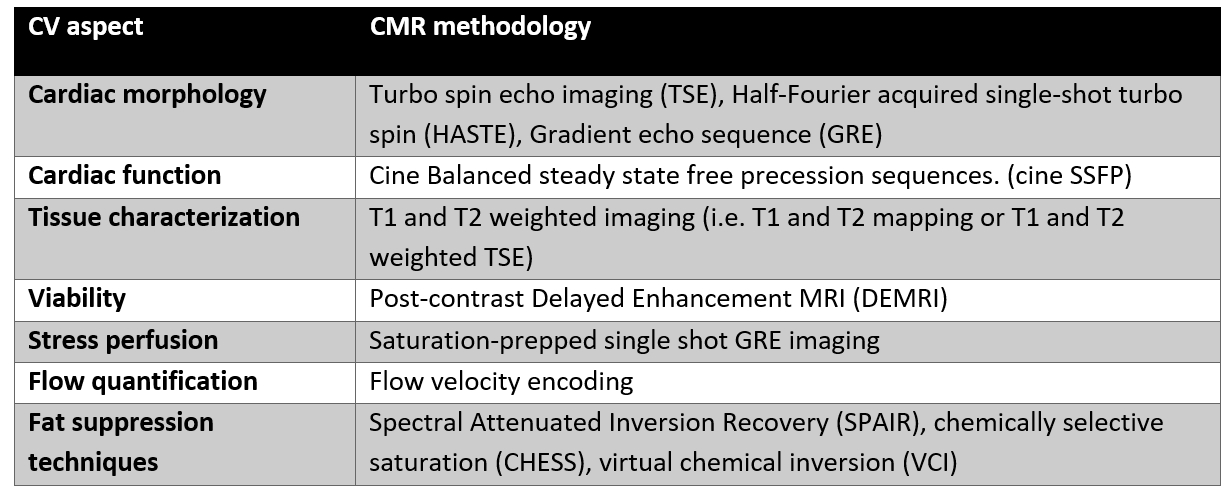
CMR imaging relies on the manipulation of signal sources in a static main magnet field by the use of radiofrequency transmission and reception for image encoding. Improvements in CMR over the past 15 years have focused on reducing scan time (compressed sensing), improving image quality (higher density coil arrays) and developing new sequences targeted at specific disease characteristics (Figure 1 and Table 1).
Some of the criticism of CMR relates to test expense; however, when one considers all the "studies" that can be performed in single exam (function, flow, stress perfusion, viability, angiography, etc.), the relative costs equilibrate in patients requiring complex assessment. Use of gadolinium contrast for CMR is contraindicated in patients with renal insufficiency and claustrophobia may pose a barrier for some patients. Although, there has been technological advancements in pacemaker compatibility with magnetic resonance imaging, CMR is still contraindicated in certain devices. CMR provides a tremendous amount of information through a single study. Excellent spatial resolution and the ability to image relationship to extracardiac structures makes CMR the modality of choice in certain cardiovascular disease groups.
Figure 1: Common CMR techniques
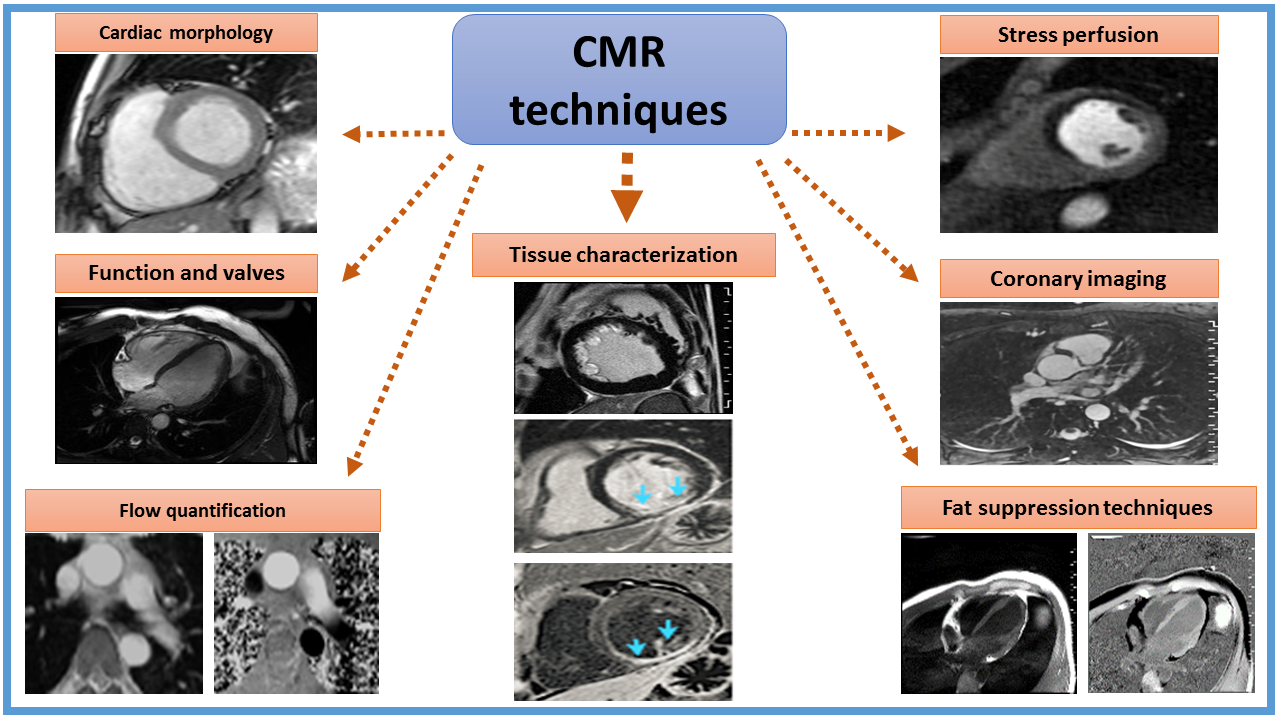
Table 1: CMR methodology for cardiovascular assessment
This article was authored by Fawaz Alenezi, MD, Fellow in Training (FIT) at Duke University in Durham, NC, and Ahmed Sami Abuzaid, MD, FACP, FACC, cardiology fellow at the University of California, San Francisco in San Francisco, CA.