Transient Effusive Constrictive Pericarditis Caused by E.Coli and E.Faecium in a Patient with a History of Esophageal Adenocarcinoma Treated with Surgery, Chemotherapy and Radiation
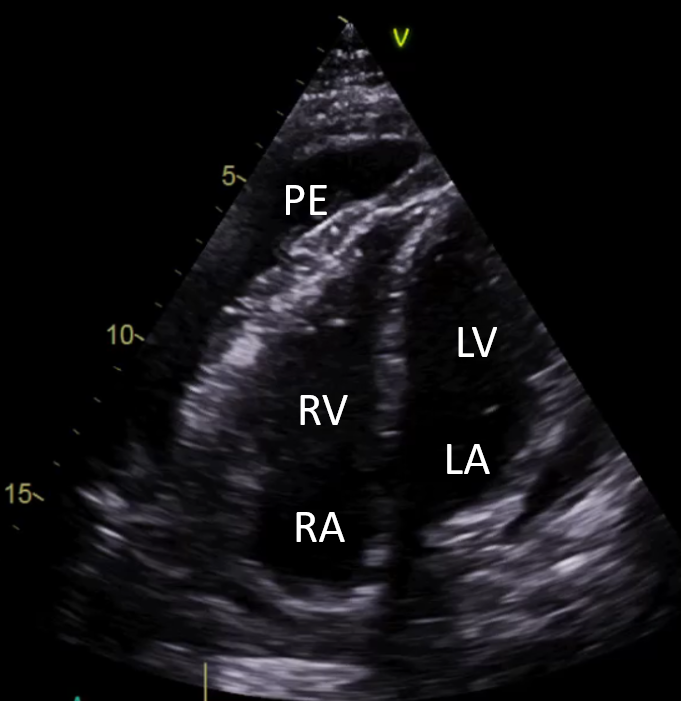
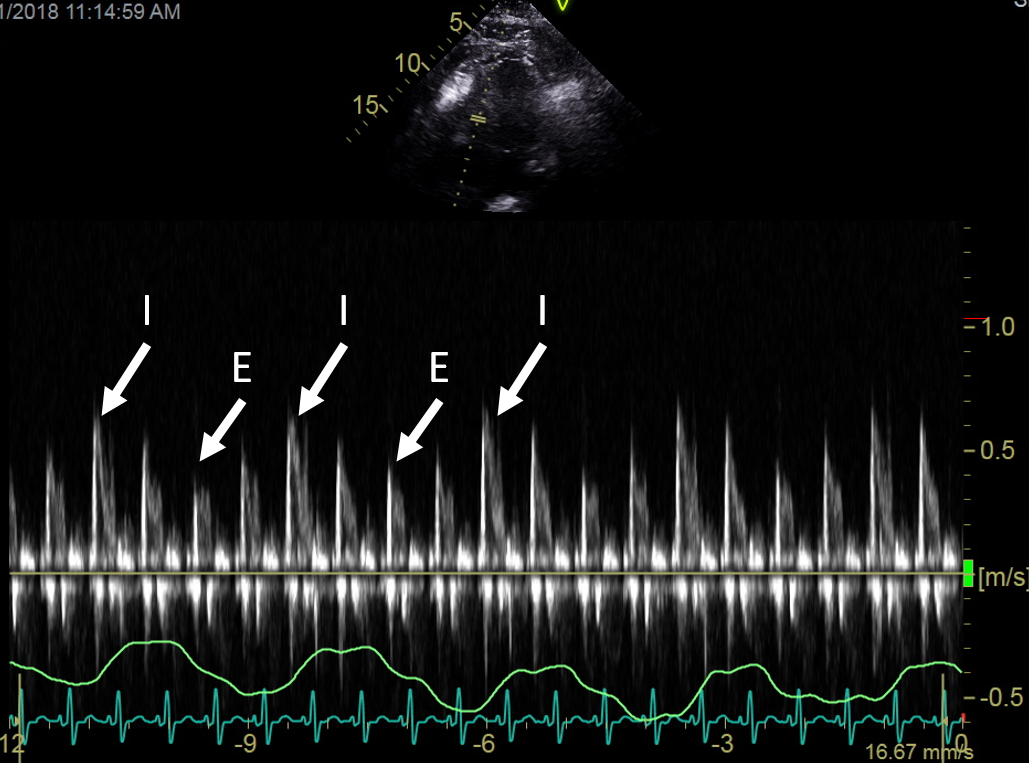
A 59-year-old male presented to the Emergency Department with two weeks duration of non-productive cough, shortness of breath and chest pressure. Past medical history included: esophageal adenocarcinoma, partial esophagectomy, chemotherapy (Carbo-Taxol) and radiation treatments along with repeated esophageal dilations due to recurrent esophageal strictures. Initial workup involved a transthoracic echocardiogram that identified a large circumferential pericardial effusion (Figure 1), respirophasic septal shift and significant mitral and tricuspid valve respiratory inflow variations (Figure 2).
Figure 1
Figure 1
Figure 1. A4 chamber view showing pericardial effusion. [Pericardial Effusion (PE), Right Ventricle (RV), Right Atrium (RA), Left Ventricle (LV), Left Atrium (LA)].
Figure 1. A4 chamber view showing pericardial effusion. [Pericardial Effusion (PE), Right Ventricle (RV), Right Atrium (RA), Left Ventricle (LV), Left Atrium (LA)].
Figure 2
Figure 2
Figure 2. Respiratory inflow variation across Tricuspid valve. [I = inspiration, E = expiration].
Figure 2. Respiratory inflow variation across Tricuspid valve. [I = inspiration, E = expiration].
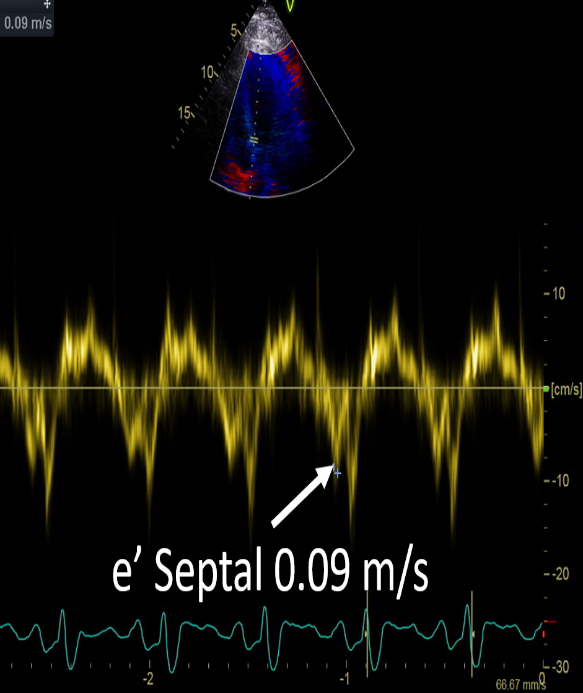
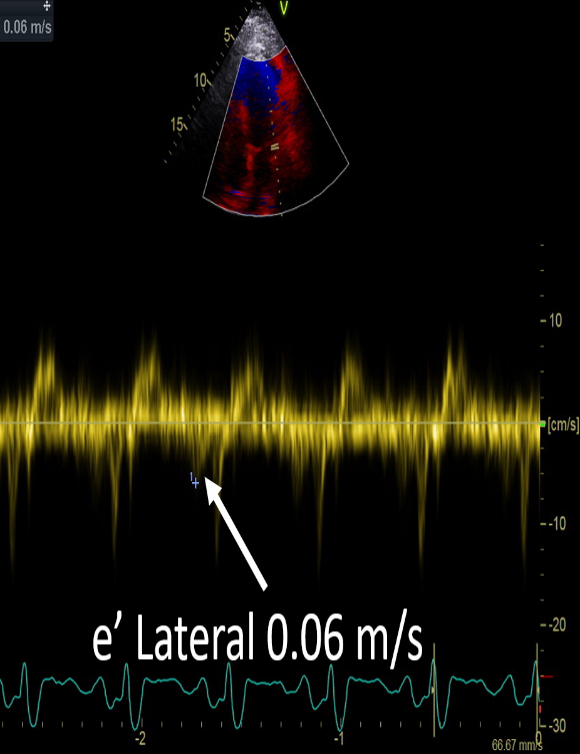
Annulus reversus was also seen. The mitral e' septal annulus tissue Doppler velocity was greater than mitral e' lateral annulus tissue Doppler velocity (Figures 3 and 4). The patient was hospitalized for further workup and management.
Figure 3
Figure 3
Figures 3 and 4. Demonstration of annulus reversus. Mitral e' septal annulus velocity 0.09 m/s. Mitral e' lateral annulus velocity 0.06 m/s.
Figure 4
Figure 4
Figures 3 and 4. Demonstration of annulus reversus. Mitral e' septal annulus velocity 0.09 m/s. Mitral e' lateral annulus velocity 0.06 m/s.
Figures 3 and 4. Demonstration of annulus reversus. Mitral e' septal annulus velocity 0.09 m/s. Mitral e' lateral annulus velocity 0.06 m/s.
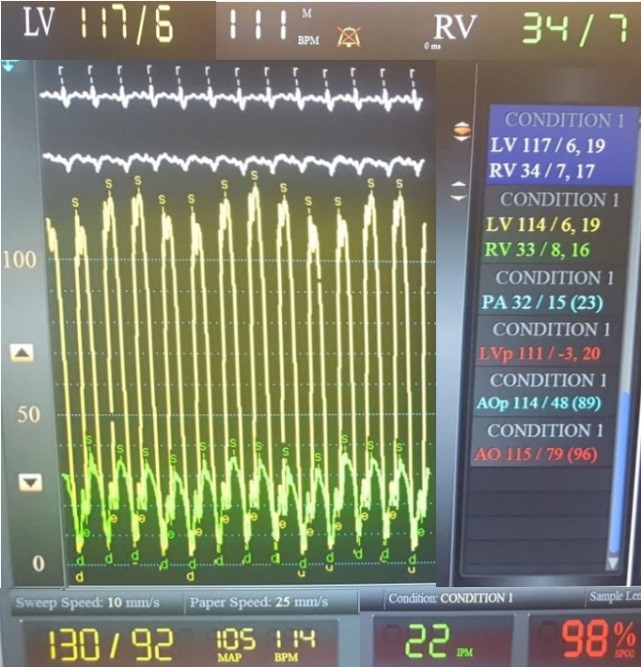
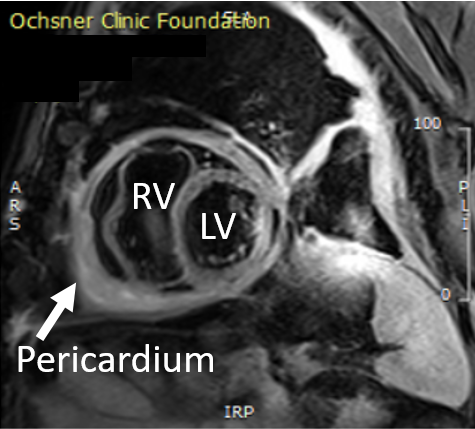
Pericardiocentesis drained sanguineous, purulent fluid that grew E.Coli and E.Faecium. Antibiotic therapy was initiated to treat bacterial pericarditis. A few days later, a cardiac catheterization was performed and showed ventricular interdependence and equalization of right and left sided diastolic pressures (Figure 5). Subsequent cardiac magnetic resonance imaging (MRI) revealed pericardial thickening and diffuse pericardial late gadolinium enhancement. It also showed prolonged myocardial relaxation time and increased signal on T2-weighted images suggestive of pericardial inflammation (Figure 6). The patient was diagnosed with effusive constrictive pericarditis.
Figure 5
Figure 5
Figure 5. Cardiac catheterization pressure tracings showing simultaneous recording of left and right ventricular pressure with similar ventricular end diastolic pressures. This is specific to constrictive pericarditis as it results from equal exerted pressure on all cardiac chambers by the fixed pericardium. Also seen is discordant respiratory variation of the left and right ventricular pressures. During inspiration, there is a rise in right ventricle filling pressure in order to maintain forward flow while there is a fall in left ventricle filling pressure. The right ventricle fills at the expense of left ventricle in the setting of a fixed pericardium. And vice versa occurs during expiration. This phenomenon, known as ventricular interdependence, is a hallmark finding in constrictive pericarditis.
Figure 5. Cardiac catheterization pressure tracings showing simultaneous recording of left and right ventricular pressure with similar ventricular end diastolic pressures. This is specific to constrictive pericarditis as it results from equal exerted pressure on all cardiac chambers by the fixed pericardium. Also seen is discordant respiratory variation of the left and right ventricular pressures. During inspiration, there is a rise in right ventricle filling pressure in order to maintain forward flow while there is a fall in left ventricle filling pressure. The right ventricle fills at the expense of left ventricle in the setting of a fixed pericardium. And vice versa occurs during expiration. This phenomenon, known as ventricular interdependence, is a hallmark finding in constrictive pericarditis.
Figure 6
Figure 6
Figure 6. Cardiovascular magnetic resonance (CMR) FS-T2 demonstrating pericardial inflammation.
Figure 6. Cardiovascular magnetic resonance (CMR) FS-T2 demonstrating pericardial inflammation.
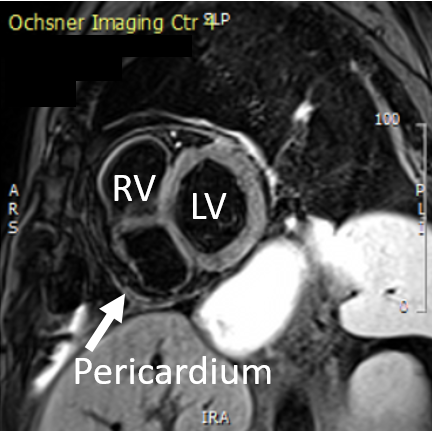
Antibiotics, colchicine, indomethacin and medical therapy for symptoms of heart failure were started. Prednisone was initiated due to marked pericardial inflammation on the cardiac MRI. A repeat transthoracic echocardiogram performed after six months on medical therapy showed resolution of the mitral and tricuspid valve inflow respiratory variations. A mild residual septal bounce was still present. Repeat cardiac MRI showed reduced pericardial inflammation (Figure 7).
The translocation of intestinal flora into the pericardial space was thought to be secondary to the repeated esophageal dilatations although no esophago-pericardial fistula was identified at that time by esophagogram, endoscopy and chest computerized tomography (CT).
Which of the following statements is correct regarding the sensitivity of the imaging modality finding used in diagnosing constrictive pericarditis (CP)?
Show Answer
The correct answer is: A. Transthoracic echocardiogram has an 87% sensitivity for diagnosing CP when there is respirophasic ventricular septal shift and medial mitral annular tissue doppler e' velocity ≥9 cm/s or ratio of expiratory diastolic hepatic vein flow ≥0.79.
Transthoracic echocardiography (TTE) is essential in evaluating patients with suspected constrictive pericarditis. In CP, there is a discordance of intrathoracic and intracardiac pressures along with intra-ventricular septal shift within a fixed space of the pericardial sac.1 During inspiration, the negative intrathoracic pressure augments right ventricular diastolic filling. The intra-ventricular septum shifts to the left ventricle given the confinement of a fixed pericardium. While in expiration, the positive intrathoracic pressure augments left ventricular diastolic filling and shifts the intra-ventricular septum to the right. Significant respiratory variation in biventricular filling occurs; there is 25-40% inspiratory decrease in mitral inflow and 40-60% inspiratory increase in tricuspid inflow.2 An important finding in CP is the annulus paradoxus in which there is a decreased mitral E/e' ratio in the presence of elevated filling pressures. There is also tethering of the lateral mitral annulus, therefore the medial annular e' is frequently higher than that of the lateral annulus. This phenomenon is known as annulus reversus, as there is a decreased motion of the lateral mitral annulus compared to the medial mitral annulus.3 Hepatic vein expiratory diastolic reversal is seen in CP. The ratio of hepatic vein diastolic reversal flow velocity over forward flow velocity in expiration is measured. Dilation of inferior vena cava is frequently seen, but it is not a specific finding in CP.
TTE has an 87% sensitivity for diagnosing CP when there is respirophasic ventricular septal shift and medial mitral annular tissue doppler e' velocity ≥9 cm/s or ratio of diastolic hepatic vein flow ≥0.79.1 The sensitivity of diagnosing CP increases to 90% when the change in tricuspid valve respirophasic inflow velocities are >45%.2 And the sensitivity of diagnosing CP becomes 100% when the change in the mitral valve respirophasic inflow velocities are >25%.2
Cardiac CT and cardiac magnetic resonance imaging (CMRI) are not initial imaging modalities used to make the diagnosis of CP, however they provide complementary information to TTE findings.3,4 Cardiac CT allows for better visualization of pericardial calcification and measurement of the pericardial thickness.2 However, only one-third of CP patients have a thickened pericardium and 25% of CP patients have evidence of pericardial calcifications.2 Due to technical difficulties with breath-holding to obtain CT images and the concern for radiation exposure, assessment for ventricular interdependence cannot be performed. Cardiac CT is more useful in the preoperative planning for pericardiectomy.2
CMRI has an 88% sensitivity in diagnosing CP.5 CMRI can also provide information regarding the anatomy and physiology of CP including ventricular interdependence, respirophasic changes in mitral and tricuspid inflow and pericardial thickening. Respiratory inflow variation with inspiration over 25% across the mitral valve and 45% across the tricuspid valve have a sensitivity of 100% and 90%, respectively, in detecting CP physiology.6 A thickened pericardium is measured with steady-state free precession (SSFP) imaging and double-inversion recovery sequence imaging.5 A radiofrequency tissue tagging sequence can evaluate the adherence of the pericardial-myocardial interface.5 CMRI can detect pericardial edema and inflammation shown by abnormal late gadolinium enhancement (LGE) on T-1 weighted images.2 Additional CMRI findings of CP include an increase in myocardial T2 relaxation time and signal intensity of T2-weighted fast spin echo images.5 LGE can be used to prognosticate CP patients. Patients with high LGE values typically respond well to anti-inflammatory therapy and are less likely to require pericardiectomy.2
Cardiac catheterization/hemodynamic evaluation is not always required but is usually confirmatory if performed. An invasive hemodynamic evaluation is still considered the gold standard for diagnosing CP.7 This assessment allows for differentiation of constrictive from restrictive pericardial disease. Constrictive pericardial disease has a restrictive ventricular filling pattern that varies with respiration.8 The 'dip and plateau pattern' or 'square root sign' is a classic finding with ventricular pressure tracings in patients with CP, which illustrates the early rapid initial filling of the ventricles and the abrupt mid to late diastolic filling when the ventricle has filled to maximum capacity set by the fixed pericardium.9 Additional findings include persistently elevated right atrial pressure even after a pericardiocentesis is performed and intrapericardial pressure has been reduced to zero.9 Also seen is elevated and equalized pressure in all four cardiac chambers.9 Cardiac catherization has a 100% sensitivity and 95% specificity of diagnosing CP if ventricular discordance is seen.9
Transient effusive constrictive pericarditis (ECP) is a reversible diseased state of thickened and inelastic pericardium in the setting of active inflammation. Incidence of ECP varies. Nowadays, doppler echocardiography has a high sensitivity and specificity for detecting constrictive pericardial physiology. Cardiac catherization is mostly pursued only when noninvasive evaluation is inconclusive. Common causes of ECP include idiopathic, active infection, connective tissue disease, and post-cardiovascular surgical changes. If ECP is diagnosed early and treated effectively, then there is a low risk of progression to chronic pericardial constriction resulting from pericardial scar formation. Transient ECP is characterized by a persistent restriction of diastolic filling after clinical pericardial tamponade is treated with a pericardiocentesis.10 Nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine and steroids are used to suppress the pericardial inflammatory state. However, if there is persistent and severe pericardial constriction, a pericardiectomy will need to be performed.
Alajaji W, Xu B, Sripariwuth A, et al. Noninvasive multimodality imaging for the diagnosis of constrictive pericarditis. Circ Cardiovasc Imaging 2018;11:e007878.
Klein AL, Abbara S, Agler DA, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease. J Am Soc Echcardiogr 2013;26:965-1012.
Brandt RR, Oh JK. Constrictive pericarditis: role of echocardiography and magnetic resonance imaging. ESC e-Journal of Cardiology Practice 2017;15:23.
Power JA, Thompson DV, Rayarao G, et al. Cardiac magnetic resonance radiofrequency tissue tagging for diagnosis of constrictive pericarditis: a proof of concept study. J Thorac Cardiovasc Surg 2016;151:1348-55.
Hoey TDE, Shahid M, Watkin RW. Computed tomography and magnetic resonance imaging evaluation of pericardial disease. Quant Imaging Med Surg 2016;6:274-84.
Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: expert recommendations. J Am Coll Cardiol 2018;72:3158-76.
Doshi S, Ramakrishnan S, Gupta S. Invasive hemodynamics of constrictive pericarditis. Indian Heart J 2015;67:175-82.
Sagrista-Sauleda J, Angel J, Sanchez A, Permanyer-Miralda G, Soler-Soler J. Effusive-constrictive pericarditis. N Engl J Med 2004;350:469-75.