A 70-year-old man with chronic lymphocytic leukemia who started ibrutinib 3 months prior is referred from the hematology clinic to cardiology with new-onset palpitations and dyspnea on exertion.
Background history includes:
Hypertension
Diabetes mellitus type II
Stage III chronic kidney disease (creatinine 1.8mg/dL)
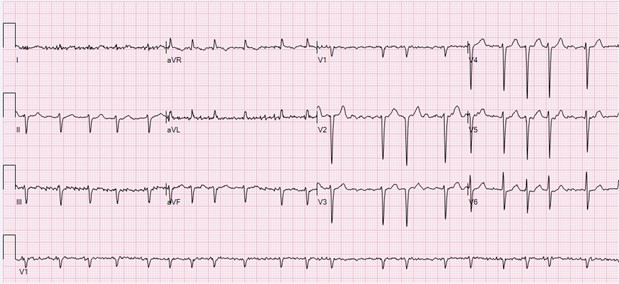
Electrocardiogram (ECG): Atrial fibrillation (AF) with rapid ventricular response at 124 bpm, nonspecific ST-T-wave abnormalities (Figure 1)
Figure 1
Figure 1
Which one of the following is the best strategy for rate control in this patient?
Show Answer
The correct answer is: A. Start metoprolol tartrate 25 mg twice daily.
Ibrutinib is associated with an increased risk of AF. Ibrutinib has many drug–drug interactions that need to be considered when selecting a rate-control agent. Ibrutinib inhibits the P-glycoprotein (P-gp) transporter and is primarily metabolized by hepatic cytochrome P450 3A4 (CYP3A4). Verapamil and diltiazem are moderate CYP3A4 inhibitors and can increase ibrutinib levels and the risk of ibrutinib toxicity. Digoxin is a P-gp substrate, and ibrutinib can increase digoxin levels and the risk of digoxin toxicity. Metoprolol does not have significant drug–drug interactions with ibrutinib and is the agent of choice for rate control in patients who develop AF with ibrutinib therapy. Although the use of nondihydropyridine calcium channel blockers (diltiazem, verapamil) is not contraindicated in patients on ibrutinib, ibrutinib doses need to be reduced in these patients to avoid toxicity. Ibrutinib should not be discontinued in patients who develop AF unless they have difficult-to-control AF or refractory heart failure.
Drs. Jennifer R. Brown, MD, PhD; John Fanikos, RPH, MBA; Michael G. Fradley, MD served as peer reviewers for this patient case.
To visit the online course page for the Management of Afib in Oncology Patients: A Case Study in CCL Treatment, click here!
References
Fancher KM, Pappacena JJ. Drug interactions with Bruton's tyrosine kinase inhibitors: clinical applications and management. Cancer Chemother Pharmacol 2020;86:507-15.
Ganatra S, Sharma A, Shah S, et al. Ibrutinib-associated atrial fibrillation. JACC Clin Electrophysiol 2018;4:1491-500.