A 70-year-old man who is affected by arterial hypertension, hyperlipidemia, severe chronic obstructive pulmonary disease treated with oxygen therapy, and known history of nonobstructive extracranial carotid artery disease is referred for a follow-up assessment of carotid artery disease.
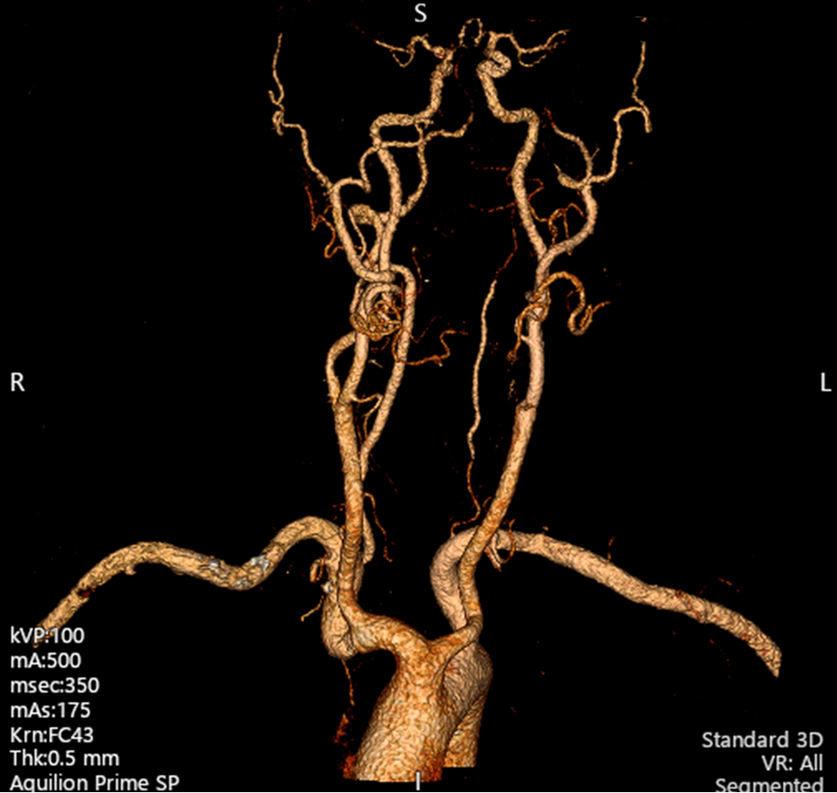
After a Doppler ultrasound carotid evaluation, a secondary-level diagnostic examination is performed. The angiography computed tomography scan detects a critical carotid stenosis of the left internal carotid artery (ICA) (Figures 1, 2).
Figure 1
Figure 1
3D CT scan of the aortic arch and supra-aortic vessels facing the origin of the BCA.
3D = three-dimensional; BCA = brachiocephalic artery; CT = computed tomography.
3D CT scan of the aortic arch and supra-aortic vessels facing the origin of the BCA.
3D = three-dimensional; BCA = brachiocephalic artery; CT = computed tomography.
Figure 2
Figure 2
3D CT scan of the aortic arch and supra-aortic vessels.
3D = three-dimensional; CT = computed tomography.
3D CT scan of the aortic arch and supra-aortic vessels.
3D = three-dimensional; CT = computed tomography.
The clinical case is therefore discussed by a multidisciplinary team that includes a vascular surgeon, interventional cardiologist, radiologist, and primary care physician (PCP). Given the high surgical risk and patient comorbidities, the team decides on an endovascular revascularization strategy.
Angiography performed by radial access confirms the left ICA critical stenosis (Video 1). A self-expandable with closed-cell design stent (WALLSTENT® 7 x 40 mm [Boston Scientific, Marlborough, Massachusetts]) is successfully implanted (Video 2).
Video 1
Video 1
Diagnostic angiography of the left ICA stenosis.
ICA = internal carotid artery.
Diagnostic angiography of the left ICA stenosis.
ICA = internal carotid artery.
Video 2
Video 2
Postprocedural angiography of the left ICA with self-expandable stent implanted.
ICA = internal carotid artery.
Postprocedural angiography of the left ICA with self-expandable stent implanted.
ICA = internal carotid artery.
The patient is discharged home on appropriate medical therapy 2 days after the procedure. He is free of symptoms and did not have any in-hospital adverse events.
Which one of the following is the anatomical feature of the aortic arch and supra-aortic vessels?
Show Answer
The correct answer is: C. Type A bovine aortic arch.
The bovine aortic arch represents the most common variant of the aortic arch, and is defined by the origin of the left common carotid artery (LCCA) off the brachiocephalic artery (BCA).1 American College of Cardiology (ACC) guidelines recognize two types of bovine aortic arch: type A, in which the LCCA arises directly from the BCA (9% prevalence in the overall population); and type B, in which both the LCCA and BCA arise from a common origin (13% prevalence in the overall population).2
This case was a type A bovine arch, as the origin of the LCCA was off the BCA (Figures 1, 2). Answer choice C is thus the correct choice, and answer choice D is an incorrect choice (the LCCA and BCA do not share a common origin).
Madhwal's anatomical classification of the aortic arch includes three types and is based on the ratio between the LCCA diameter and the vertical distance from the top of the aortic arch to the BCA origin. A type I aortic arch is defined as a smaller aortic arch–to-BCA distance than the LCCA diameter (ratio <1). A type II arch is defined as the aortic arch–to-BCA distance being one to two times that of the LCCA diameter. A type III aortic arch is defined as the distance being more than two times the LCCA diameter.3
Answer choices A and B are incorrect choices because this patient did not meet the criteria for a type II or III aortic arch according to Madhwal's classification (Figure 1).4 Answer choice E is an incorrect choice because his right VA origin was from the right subclavian artery. An aberrant origin of the VA is a less common anatomical variant of the aortic arch in which the VA originates from either the aortic arch, common carotid artery, ICA, or external carotid artery.
An important management aspect of this case was the challenge of revascularization in a patient with a bovine arch. Appropriately, a multidisciplinary team approach was used. Surgical revascularization was deemed unfeasible because of the unfavorable risk/benefit balance, including operative and postoperative risk. The participating radiologist and interventional cardiologist concurred that a less invasive approach was technically feasible despite the bovine arch structure. Finally, the PCP reviewed this information and agreed with the recommendation to proceed with an endovascular approach. On the basis of local catheterization laboratory expertise, an endovascular strategy via right radial artery access was preferred to approaching the left ICA stenosis. In a published cohort of 176 patients with bovine arch, the endovascular approach for carotid stenosis was safe, with a success rate of 96%.5
References
Shapiro M, Raz E, Nelson PK. Aortic arch variants: a practical guide to safe and timely catheterization. Interv Neurol 2018;7:544-55.
Isselbacher EM, Preventza O, Hamilton Black J III, et al.; Writing Committee Members. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2022;80:e223-e393.
Marrocco-Trischitta MM, Glauber M. Implications of different definitions for aortic arch classification provided by contemporary guidelines on thoracic aortic repair. Interact Cardiovasc Thorac Surg 2021;32:950-2.
Bae SB, Kang EJ, Choo KS, et al. Aortic arch variants and anomalies: embryology, imaging findings, and clinical considerations. J Cardiovasc Imaging 2022;30:231-62.
Casana R, Bissacco D, Malloggi C, et al. Aortic arch types and postoperative outcomes after carotid artery stenting in asymptomatic and symptomatic patients. Int Angiol 2020;39:485-91.