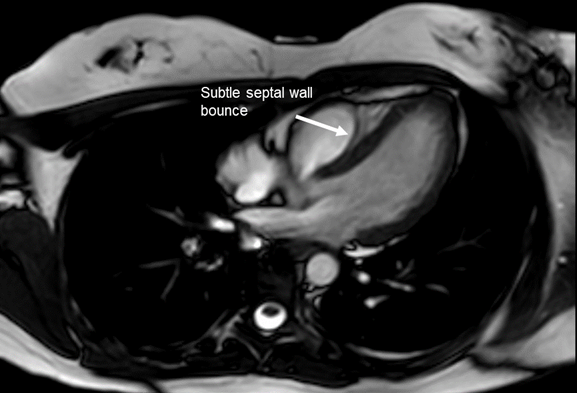
The patient is a 29-year-old gravida 1 para 0 woman with a history of chronic idiopathic recurrent pericarditis who presents for further evaluation of her pericardial disease. She was first diagnosed with pericarditis approximately 3 years ago with symptoms manifesting as positional and pleuritic chest pain. Various combination therapies involving colchicine, ibuprofen, azathioprine, and prednisone either failed to remit her symptoms or were associated with intolerable side effects. She has never demonstrated imaging evidence of constriction. She reports ongoing pericardial chest pain. Laboratory analysis is notable for elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). An initial transthoracic echocardiogram (TTE) followed by a cardiac magnetic resonance imaging (MRI) demonstrates findings shown below (Figures 1 – 5).
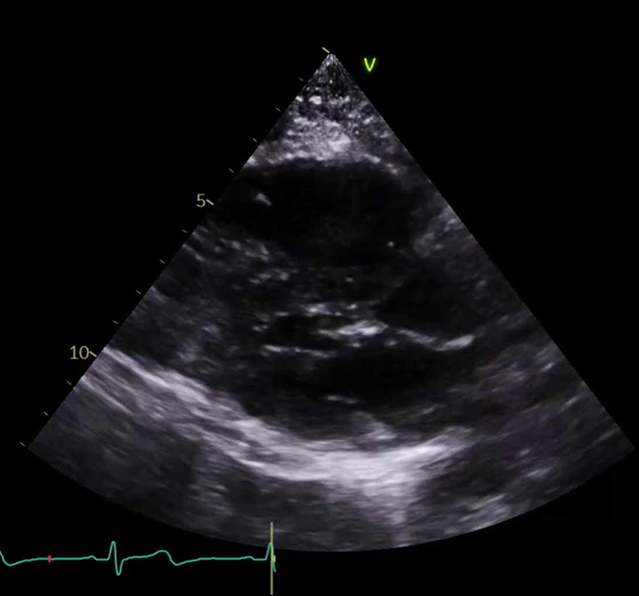
Figure 1
Figure 1
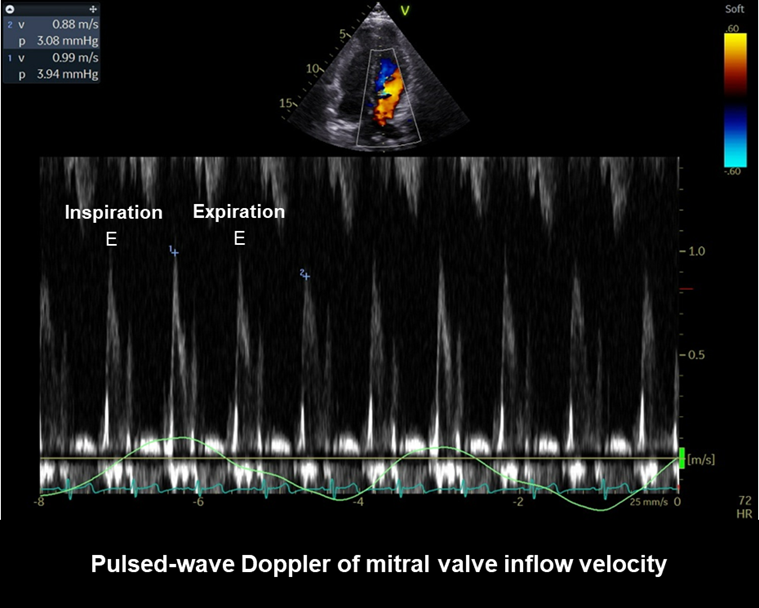
Figure 2
Figure 2
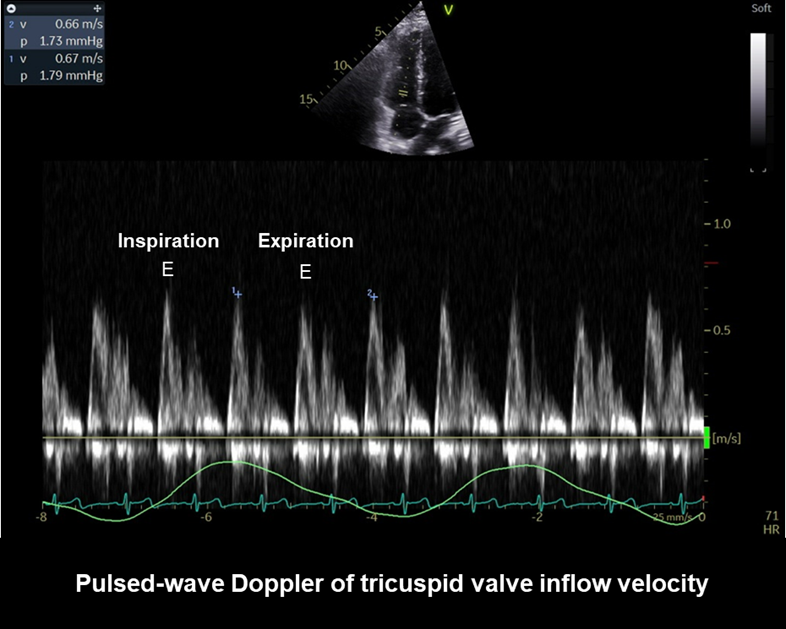
Figure 3
Figure 3
Figure 4
Figure 4
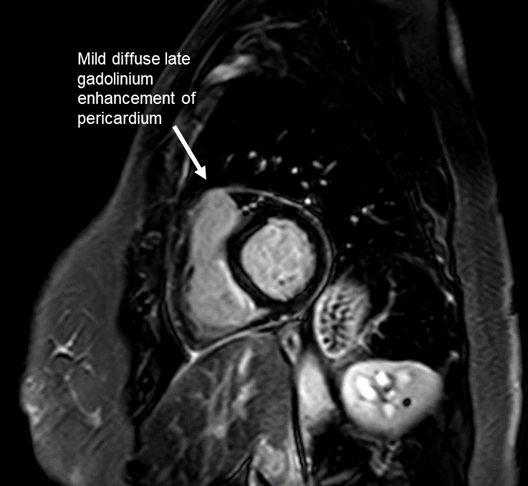
Figure 5
Figure 5
She notes to you today that she is also pregnant at 10 weeks gestation. She is currently taking colchicine 0.6 mg twice daily and ibuprofen 600 mg three times daily.
Which of the following is the most appropriate next step in the management of her pericarditis?
Show Answer
The correct answer is: A. Initiate anakinra with referral to high-risk obstetrics and maternal fetal medicine referral.
Anakinra is an interleukin-1 (IL-1) inhibitor therapy that has demonstrated efficacy the management of inflammatory chronic pericarditis (with elevated inflammatory markers and late gadolinium enhancement [LGE] in Figure 5 ). IL-1 blockade therapy was not conventionally supported for use in pregnancy. However, limited safety data regarding the use of IL-1 inhibitor therapy among pregnant women has not been associated with adverse perinatal or patient outcomes. According to the European Alliance of Associations for Rheumatology, anakinra can be used before and during pregnancy when no other therapeutics are able to remit disease. There is no available safety data on the use of rilonacept during pregnancy.1 When initiating this therapy for refractory pericarditis, shared decision-making is paramount along with multidisciplinary consultation with maternal fetal medicine, obstetrics, and cardiology.
High dose aspirin would not be an acceptable next step in management in this pregnant patient. Use of high doses of aspirin during pregnancy can be associated renal hypoperfusion and oligohydramnios as well as premature closure of the ductus.1
Initiation of steroid therapy would not be appropriate in this patient as she had been trialed on steroids in the past without success.2
Mycophenolate mofetil is known to be highly teratogenic and has been associated with miscarriage and malformation. Though it has some limited utility in pericarditis, it would not be acceptable use in this pregnant patient.1
As this patient reports ongoing chest pain with elevated inflammatory markers and ongoing LGE on cardiac MRI, the next step in therapy would require escalation of therapy to IL-1 blockade. Colchicine is acceptable to use in all stages of pregnancy and ibuprofen at up to 20 weeks gestation.2
References
Serati L, Mardigyan V, Caccia Dominioni C, et al. Pericardial diseases in pregnancy. Can J Cardiol 2023;39:1067-77.