STEMI at Elderly Age (Part Two)
Which of the following would be the optimal management for this patient?
Show Answer
The correct answer is: B. Acute PCI with stenting.
After discussing the risks and benefits with the patient and the family, both agree to diagnostic coronary angiography with intent for percutaneous coronary intervention (PCI) reperfusion with stenting. She is treated with aspirin, clopidogrel and unfractionated heparin (weight-based dosing) and urgently transported to the cardiac catheterization laboratory. Beta blocker therapy is deferred due to the increased risk of shock with intravenous beta blockers. An angiotensin-converting-enzyme (ACE) inhibitor and a high-intensity statin are administered.
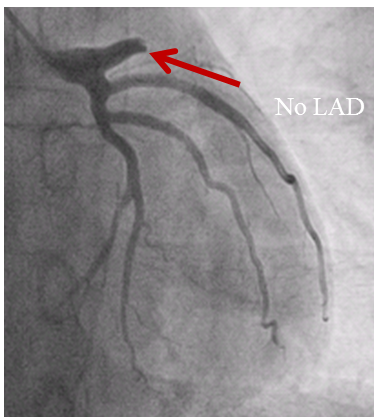
Coronary angiography shows complete proximal left anterior descending artery occlusion (Figure 2).
Figure 2: Pre-PCI Coronary Arteriogram
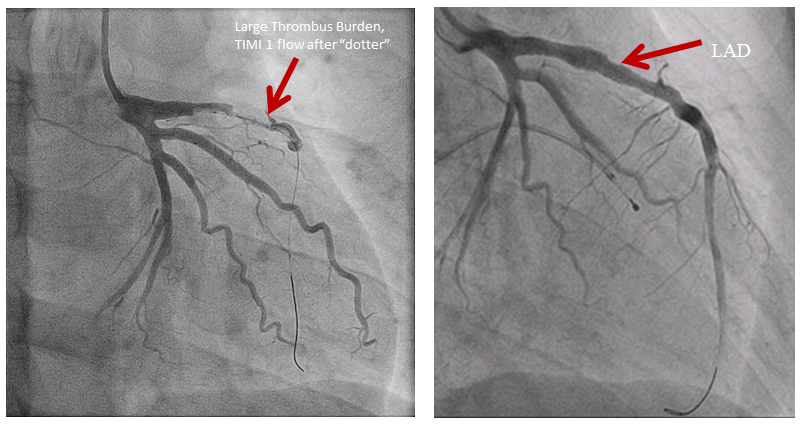
At cardiac catheterization there was a sizeable clot burden and sluggish flow. A bare metal stent restored flow in the left anterior descending coronary artery. To minimize complications, a 75% lesion in the mid RCA was not intervened on. The post procedure blood pressure was 140/90 mm Hg and the patient is transferred to the Coronary Care Unit.
The procedural arteriogram is shown (Figure 3).
Figure 3: PCI Procedural Arteriogram
Answer choice A is incorrect as PCI is favored over thrombolytic therapy because of the lesser risk of hemorrhagic stroke. In addition, thrombolytic therapy is associated with an increased risk of myocardial rupture at age beyond 75 years (17% vs. 5% with PCI).
Answer choice B is correct because PCI is favored over thrombolytic therapy (at least to age 80) because it decreases 30-day mortality, and there is particular benefit in patients with anterior myocardial infarction. The major benefits of primary PCI with stenting are a decrease in recurrent ischemic events and decreased need for subsequent target vessel revascularization.
Answer choice C is incorrect because although PCI provides benefit, the balloon dilatation provides less satisfactory short- and long-term outcomes than stenting. The presence of an acute STEMI mandates dual anti-platelet therapy (DAPT), optimally for one year—so that the lesser duration DAPT with balloon dilatation than with stenting is not relevant for this patient.
Answer choice D is incorrect. "Time is muscle"—the major benefit in patients in all ages with ST elevation myocardial infarction is immediate myocardial revascularization, optimally within the initial 60-90 minutes after presentation to the Emergency Department.
Answer choice E is incorrect because this patient is an active, alert and independent older adult, has no specific contraindications to PCI, and medical therapy is reserved only for those patients with anticipated shortened lifespan, complicating multi-morbidities, and those for whom PCI and its consequent therapy is inappropriate.
References
- Bueno H, Betriu A, Heras M, et al. Primary angioplasty vs. fibrinolysis in very old patients with acute myocardial infarction: TRIANA (TRatamiento del Infarto Agudo de miocardio eN Ancianos) randomized trial and pooled analysis with previous studies. Eur Heart J 2011;32:51-60.
- O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;61;485-510.
- Alexander KP, Newby LK, Armstrong PW, et al. Acute coronary care in the elderly, part II: ST-segment-elevation myocardial infarction: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: In collaboration with the Society of Geriatric Cardiology. Circulation 2007;115:2570-89.
- Saunderson CE, Brogan RA, Simms AD, Sutton G, Batin PD, Gale CP. Acute coronary syndrome management in older adults: guidelines, temporal changes and challenges. Age Ageing 2014;43:450-5.
- Veerasamy M, Edwards R, Ford G, et al. Acute coronary syndrome among older patients: a review. Cardiol Rev 2015;23:26-32.
- Grosmaitre P, Le Vavasseur O, Yachouh E, et al. Significance of atypical symptoms for the diagnosis and management of myocardial infarction in elderly patients admitted to emergency departments. Arch Cardiovasc Dis 2013;106:586-92.
- Newell MC, Henry JT, Henry TD, et al. Impact of age on treatment and outcomes in ST-elevation myocardial infarction. Am Heart J 2011;161:664-72.