Focus on EP | Value of Cardiac EPs in Perioperative Cardiac Surgical Care

An invitation to speak recently on the role of cardiac electrophysiologists (EPs) in perioperative care, at the annual meeting of the Florida Society of Thoracic and Cardiovascular Surgeons, led me to reflect on my interactions with cardiothoracic surgeons (CTS). I realized that EPs and CTS are often siloed in our clinical practices: I typically only seek the help of CTS for postoperative complications and CTS only seek my support if postoperative arrhythmic issues arise.
In contrast, my interventional and structural cardiology colleagues routinely involve CTS in the preprocedural management of complex coronary interventions, transcatheter aortic valve replacements and transcatheter mitral valve repair. The dependency between EP and CTS is largely reactive, not proactive in nature, and this does not seem like an optimal relationship for providing the best possible care for patients.
As the field of medicine becomes more multidisciplinary and prevention focused, I propose that EPs become more collaborative with CTS in identifying and managing arrhythmic conditions. While the concept of shared decision-making is largely between patients and their clinicians, I believe that shared decision-making between clinicians, including EPs and CTS, can similarly improve clinical outcomes and patient satisfaction. Here are several examples of perioperative management scenarios where EPs can provide value to their CTS colleagues.
High-Risk AV Block
The most challenging permanent pacemaker implants often occur in the immediate postoperative setting in cardiac surgery patients who are 1) at high risk of bleeding due to recent anticoagulation and antiplatelet treatment, 2) at high risk of infection due to postoperative systemic inflammation, or 3) hemodynamically tenuous but dependent on a temporary pacing wire. This is often the case after cardiac valvular interventions, which are prone to causing atrioventricular (AV) block.
We can predict the risk for a postoperative pacemaker implant based on evidence from Koplan, et al., who developed a simple risk score, namely, age >70 years, atrial fibrillation (AFib), prolonged PR, bundle branch block, prior valve surgery and need for multivalvular surgery.1
Patients with four or more of these clinical features are at high risk, with a 25% incidence of pacemaker implant in the study, and those with all six features have a 50% incidence of pacemaker implant.
For these high-risk patients, it would be reasonable to involve EPs preoperatively to arrange for an intraoperative leadless pacemaker implant. This can prevent the need to implant a temporary pacing wire or the need to implant a postoperative permanent pacemaker, which can ultimately shorten the length of hospitalization.
Oates, et al., recently described the long-term safety and efficacy of intraoperative leadless pacemaker implant at the time of valve surgery in 100 consecutive patients, the majority of whom had prophylactic indications for pacemaker implant (Figure 1).2
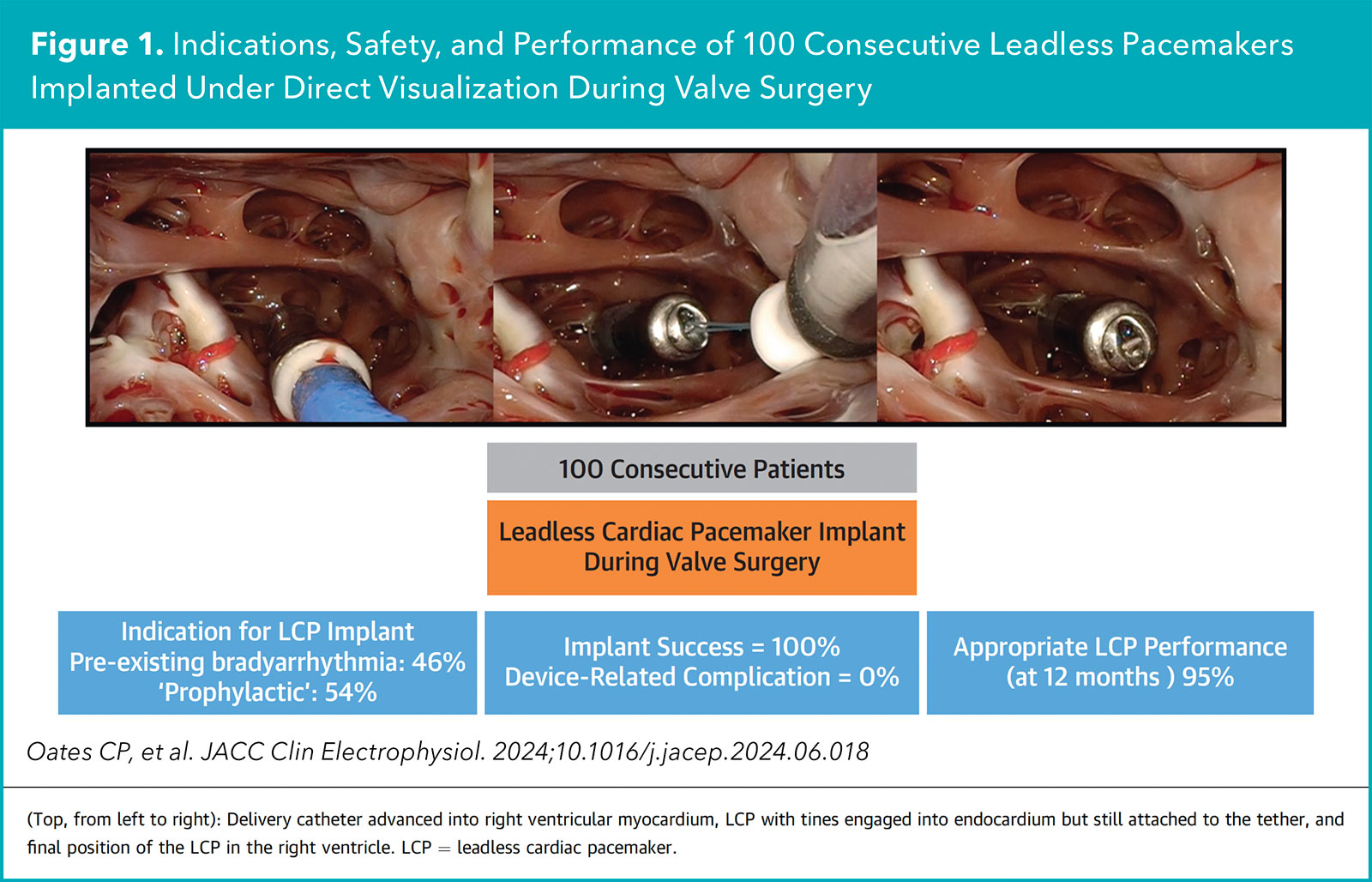
The leadless pacemaker was successfully implanted in all cases without device-related complications. At 12 months, the pacing threshold was acceptable in 95% of patients.
Atrial Fibrillation/Flutter
In patients with AFib and atrial flutter (AFL) who are undergoing cardiac surgery, the 2023 ACC/AHA guideline for AFib has emphasized concomitant left atrial appendage occlusion (class I recommendation), posterior left pericardiotomy (class 2A recommendation) and surgical ablation (class 2A recommendation).3
The current cardiothoracic surgery guidelines do not include these new ACC/AHA recommendations and it's likely that most CTS are not aware of them. Therefore, EPs can serve as an advocate for these recommendations to help best serve patients by not missing the intraoperative opportunity to address AFib.
Specifically for surgical ablation, the extent of ablation can vary depending on the nature of the arrhythmia and not all patients may require a complete Cox-Maze biatrial lesion set. Insufficient ablation may result in inadequate arrhythmia control and excessive ablation can be pro-arrhythmic.
EPs can guide CTS in clarifying the arrhythmia diagnosis, distinguishing AFib from AFL, and recommending the most relevant surgical lesion sets based on the suspected substrate and mechanism. This can be particularly helpful in patients with persistent AFib, prior AFib ablation and atypical AFL, who would benefit from more than just pulmonary vein isolation.
Ventricular Arrhythmias
In select patients undergoing cardiac surgery who have clinically significant premature ventricular contractions (PVCs) originating from a surgically accessible anatomical site, it may be reasonable to pursue concomitant intraoperative surgical ablation.
EPs can review the electrocardiogram signature of the PVC to localize the suspected site of origin, providing a "map" to guide CTS to the myocardial substrate that should be targeted. Case reports have described surgical ablation of PVCs originating from the left ventricular outflow tract and from the papillary muscles.4,5
El-Eshmawi, et al., described three patients with papillary muscle-PVC associated with ventricular tachycardia or ventricular fibrillation who underwent concomitant intraoperative surgical cryoablation of the culprit papillary muscle at the time of elective mitral valve repair for severe mitral regurgitation (Figure 2).5
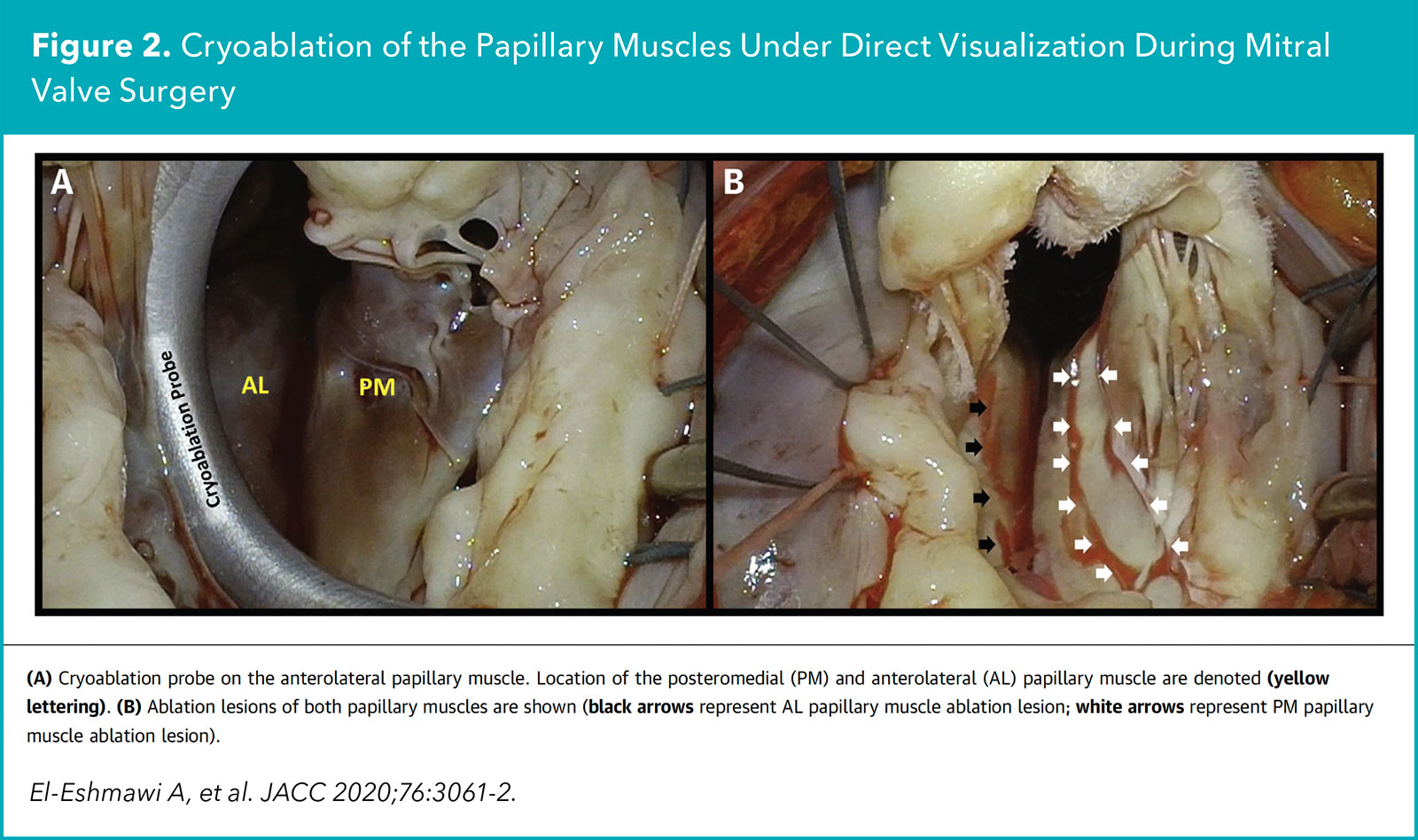
At three to six months follow-up, repeat Holter monitoring demonstrated a median PVC reduction of 97.9% and repeat transthoracic echo demonstrated minimal mitral regurgitation.
Postoperative AFib
Postoperative AFib after cardiac surgery is associated with increased perioperative renal failure, myocardial infarction, stroke and mortality, as well as long-term progression to persistent AFib, stroke and mortality.6 Not surprisingly, the management of postoperative AFib is a priority for the Enhanced Recovery after Cardiac Surgery initiative.7
Of note, whether AFib is preexisting or newly onset after cardiac surgery, it ultimately progresses over time, similar with other chronic cardiovascular conditions, and often requires long-term treatment with anticoagulants, antiarrhythmic drugs and ablation.
Again, in this setting, EPs could partner early on with CTS in the perioperative inpatient management of AFib and continue to provide longitudinal care in the outpatient setting – thereby reducing morbidity and mortality related to postoperative AFib, as well as adverse events associated with long-term medication use, particularly from anticoagulants and antiarrhythmic drugs.
Looking Ahead
At the meeting, I had a fantastic time exploring the numerous ways that EPs and CTS can improve patient-focused care and patient outcomes by collaborating and enhancing each other's practice. From lead extractions to the convergent hybrid procedure to inappropriate sinus tachycardia ablation, there seems to be no shortage of scenarios where patients could benefit from the multimodality approach provided by an EP and CTS partnership. I look forward to greater collaboration with my CTS colleagues and I encourage other EPs to consider the same.

This article was authored by Edward Chu, MD, FACC (@Ed_Chu_MD), an electrophysiology attending physician in Miami, FL.
References
- Koplan BA, Stevenson WG, Epstein LM, Aranki SF, Maisel WH. Development and validation of a simple risk score to predict the need for permanent pacing after cardiac valve surgery. J Am Coll Cardiol 2003;5;41:795-801.
- Oates CP, Breeman KTN, Miller MA, et al. Long-term safety and efficacy of intraoperative leadless pacemaker implantation during valve surgery. JACC Clin Electrophysiol 2024;Aug 1:S2405-500X(24)00634-0.
- Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation. J Am Coll Cardiol 2024;83:109-279.
- Choi EK, Nagashima K, Lin KY, et al. Surgical cryoablation for ventricular tachyarrhythmia arising from the left ventricular outflow tract region. Heart Rhythm 2015;12:1128-36.
- El-Eshmawi A, Pandis D, Miller MA, et al. Surgical cryoablation of papillary muscle PVCs during mitral valve surgery: Therapeutic consideration for malignant MVP. J Am Coll Cardiol 2020;76:3061-2.
- Caldonazo T, Kirov H, Rahouma M, et al.; POAF-MA Group. Atrial fibrillation after cardiac surgery: A systematic review and meta-analysis. J Thorac Cardiovasc Surg 2023;165:94-103.e24.
- Grant MC, Crisafi C, Alvarez A, et al. Perioperative care in cardiac surgery: A joint consensus statement by the Enhanced Recovery After Surgery (ERAS) Cardiac Society, ERAS International Society, and The Society of Thoracic Surgeons (STS). Ann Thorac Surg 2024;117:669-89.
Clinical Topics: Arrhythmias and Clinical EP, Cardiac Surgery, Invasive Cardiovascular Angiography and Intervention, Implantable Devices, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Cardiac Surgery and Arrhythmias
Keywords: Cardiology Magazine, ACC Publications, Perioperative Care, Electrophysiology, Transcatheter Aortic Valve Replacement, Atrial Fibrillation, Pacemaker, Artificial