For the FITs | High Cost of Heart Failure Treatment: Stories From the Frontline

Guideline-directed medical therapy (GDMT) is essential for managing heart failure with reduced ejection fraction (HFrEF). The 2022 ACC/ AHA/HFSA guideline on the management of HF recommends using renin-angiotensin-aldosterone system inhibitors with a preference for angiotensin receptor-neprilysin inhibitors (ARNIs), beta-blockers, mineralocorticoid receptor antagonists, and sodium glucose cotransporter 2 (SGLT2) inhibitors to improve survival, symptoms, ventricular function and quality of life.1
Despite these recommendations, implementing these therapies in real-world settings is challenging, with financial toxicity being a prominent reason that often creates an odyssey for many patients, particularly those who are disadvantaged.
The introduction of new medications like ARNIs and SGLT2 inhibitors, while leading to substantial reductions in mortality and improvements in symptoms, has significantly increased out-of-pocket costs for patients, with well-insured Medicare patients facing annual expenses as high as $2,849.2
The situation is even more dire for those who are underinsured or uninsured, making access to these lifesaving therapies difficult for the most vulnerable populations.
Financial Barriers to GDMT

SGLT2 inhibitor medications have steep retail prices, with empagliflozin costing more than $600 and sacubitril/valsartan more than $700 for a month's supply.3,4 These prices are prohibitive for patients without insurance, leading to either financial disaster or just outright skipping this important life-preserving therapy.
As stated by Gunn and Pendyal in their paper on the risk of financial toxicity with novel cardiovascular treatments, "perhaps unsurprisingly, this high financial burden is inequitably distributed."5
In fact, in a study involving patients with HFrEF and their families, those with low incomes faced a catastrophic financial burden from medical expenses at a rate up to 10-times higher than that of middle- and high-income families.6
Furthermore, this burden disproportionately affects Black patients, who experience financial difficulties from medical bills at a rate 50% higher than White patients, even after accounting for differences in education, insurance coverage and geographical location.7
The high costs of these medications also contribute to physician inertia in prescribing them, as many insurances require prior authorization, impeding early initiation and decreasing patient adherence.8
This begets the question: What is the value of therapies that have reduced HF mortality, from a rate of 40-50% before we had the current guideline-directed drugs to now around 10% with all four recommended drugs, if people cannot obtain them?
Often those who cannot obtain them are those who need the therapy the most.
Prior Authorization
Prior authorization is a significant barrier, leading many physicians to avoid prescribing necessary therapies and many patients to abandon hope of obtaining needed medications. Stories of patients spending hours on the phone every time there's a medication change and waiting months to get a new medication approved are common.
It's a process that wastes the physician's and the patient's time in an effort to stagnate the prescription of costly medications. Many such stories can be found at fixpriorauth.org. In many practices, ancillary staff are hired solely to manage prior authorizations, an extremely time-consuming task.
As a cardiology fellow seeing disadvantaged patients without such support, I've experienced the nightmare of providing these medications to patients with insurance. Multiple phone calls lasting 15 to 30 minutes to insurance companies or pharmacies are common, often providing the same information repeatedly.
This situation raises the question: How many physicians opt not to prescribe these therapies due to these barriers? From the patient's perspective, how many give up on obtaining these medications due to the hurdles they face?
A Patient's Struggle

In my clinic, I encountered a patient whose story exemplifies the hardships faced by many in accessing essential medications. This patient, a racial/ethnic minority, recently released from jail, was diagnosed with new-onset HFrEF with a left ventricular ejection fraction of 15% due to nonischemic cardiomyopathy. He presented with severe NYHA class IV symptoms.
Despite his grim initial presentation, he had remarkable improvement with the initiation of all four pillars of GDMT. However, his progress was jeopardized when he could no longer afford empagliflozin and sacubitril/valsartan because his insurance did not cover them.
Struggling to find a job post-incarceration, the patient was devastated and came to my office in tears, not knowing how to continue his treatment. We consoled him and provided him with samples to bridge the gap while we worked towards a solution. Later, we discovered he could obtain these medications from Canada, through a family member living there, at a lower cost but required a prescription, which we provided.
We are currently working with the patient to switch him to a different more comprehensive insurance carrier that will cover his medications. While this patient did not give up and was able to obtain his medications, it underscores the lengths patients must go to access necessary treatments and the systemic issues that need addressing.
Sadly, many patients are not able to go to such lengths. Some might be the family's breadwinner and are barely able to obtain time off for medical appointments, much less to spend three hours on the phone with the insurance company or travel to another country to obtain medications.
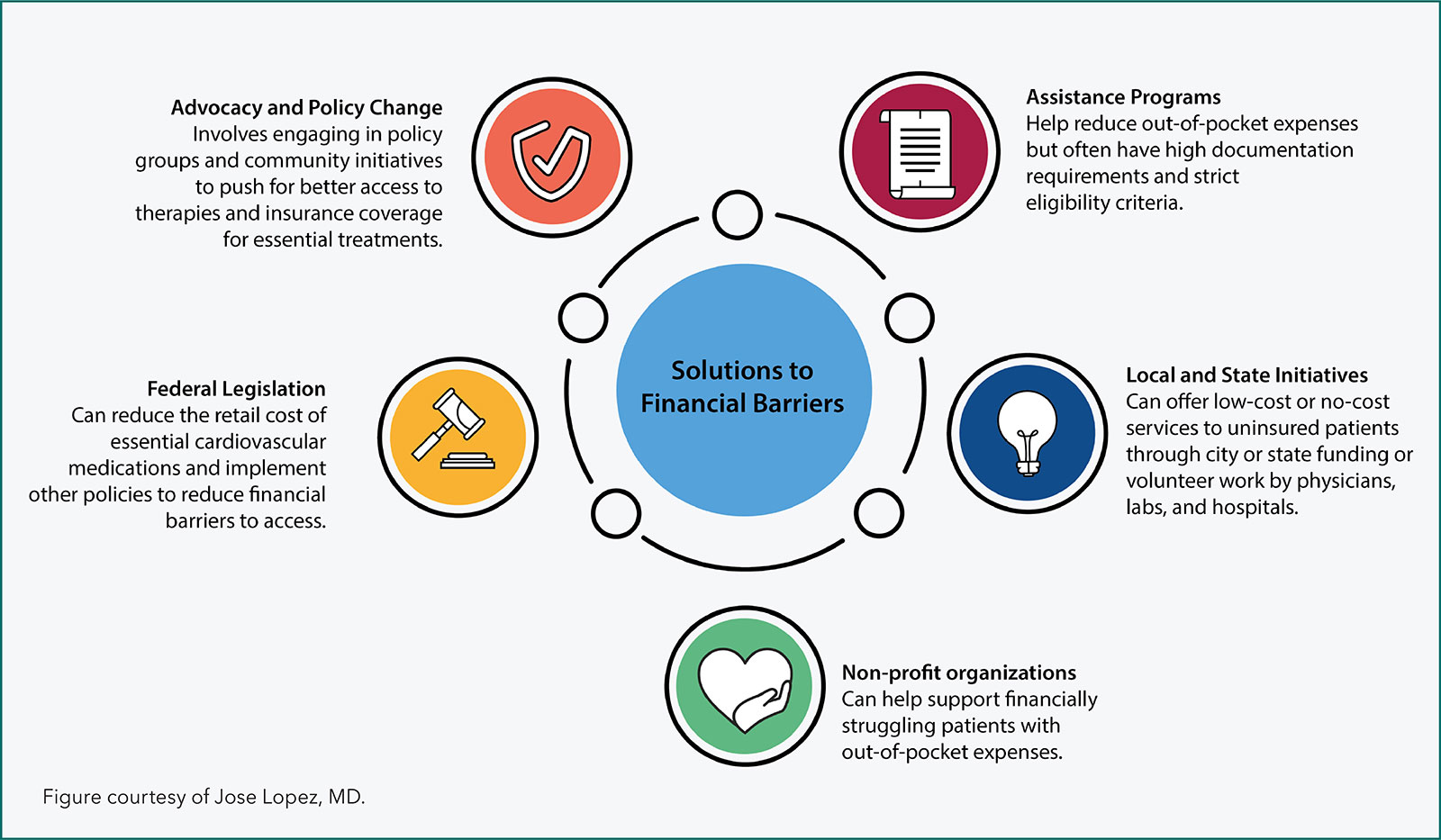
Current Solutions
Several resources are available to help bridge disparities in access to medical therapies. For many practicing clinicians, referring patients to assistance programs or providing co-payment coupons has been a practical solution to offset the high costs of newer medications.5
However, as described by Gunn and Pendyal, this approach is frequently hindered by burdensome application procedures, extensive documentation requirements, strict income thresholds, and rigid exclusion criteria.5 Consequently, these solutions often serve as temporary remedies rather than sustainable, long-term solutions.
Click here to read more about the recently announced results of the Medicare Drug Negotiation Program negotiation, with agreed discounts ranging from 38-79% off list price.
In Palm Beach County, FL, where my fellowship is based, the Palm Beach County Medical Society launched an initiative in 2005 called "Project Access."9 This initiative involves a network of doctors, hospitals, labs and imaging services that volunteer their time and resources for free to provide comprehensive care at no cost to uninsured patients. Once enrolled, patients receive free access to labs, imaging and physician referrals within the network.
Since its inception, Project Access has facilitated thousands of appointments and assisted over 2,400 residents, ensuring timely and appropriate care. By highlighting the structure and successes of this initiative, we can demonstrate the potential of local efforts to alleviate health care barriers.
Another significant resource available in New York is the NYC Health + Care program, a city-funded program providing low-cost and no-cost services to uninsured New Yorkers who either do not qualify for or cannot afford insurance. This program, part of the NYC Health + Hospital system, offers comprehensive medical services, including medications such as ARNIs, GLP-1RAs, and SGLT2 inhibitors, at no cost to patients.
A colleague in New York shared that some patients from other states travel specifically to New York to access these medications, bypassing residency requirements by using a local address from a close friend or family.
However, these stories paint the picture of the grim reality of health care disparities, where patients go to extreme lengths, such as crossing state lines and incurring travel costs, to secure lifesaving treatments. It also illustrates how being underinsured can be more challenging than being uninsured, such as my patient's case.
Finally, The Equity in Heart Transplant Project is an important grassroots effort in which I'm involved.10 This initiative supports patients eligible for heart transplants but unable to afford the out-of-pocket costs.10 To date, the Project has helped 31 patients, assisting them with an array of financial obstacles such as transportation, medications, insurance deductibles, child care and other unmet needs.10
At the federal level, the Inflation Reduction Act of 2022 represents a significant legislative effort to address out-of-pocket costs for Medicare beneficiaries.5,11 Starting in 2025, this legislation will cap annual medication costs at $2,000 for Medicare recipients.11
Additionally, the Medicare Drug Negotiation Program has negotiated directly with pharmaceutical companies to lower drug prices, with cardiovascular drugs being five of the 10 initial selected initially (apixaban, dapagliflozin, empagliflozin, rivaroxaban, and sacubitril-valsartan).5
While this is a positive step forward for Medicare patients, significant gaps remain for those who are uninsured or underinsured. This initiative, however, highlights the potential impact of federal policy changes and underscores the need to advocate for broader, more inclusive solutions.
Broader Context
The hurdles faced by my patient in obtaining medications proven in clinical trials and endorsed with the highest level of evidence in clinical guidelines are not isolated. Across the U.S., many patients encounter similar situations, and many give up on their health due to the difficulties in obtaining appropriate medical care.
As fellows in training (FITs) in cardiology, we must advocate for better access to therapies. This includes pushing for policy changes to ensure insurance coverage for essential diagnostic resources, medications, procedures, and supporting community-based initiatives. This can be done by involving ourselves in policy groups, leading a local initiative for disadvantaged patients, learning our community resources, and proposing and implementing solutions to bridge disparities.
Conclusion
My patient's story exemplifies that even with insurance, those who most need care often face the greatest obstacles in the pursuit of equitable care. Such stories underscore the urgent need for systemic changes, including the elimination of barriers like prior authorizations and ensuring adequate insurance coverage for guideline-recommended treatments.
Grassroots initiatives like Project Access, NYC Health + Care, and The Equity in Heart Transplant Project offer valuable frameworks for developing similar programs in other regions facing comparable challenges. Federal policy changes that benefit all patients, not just those covered by a certain insurance, are imperative.
As future leaders in cardiology, FITs have a critical role in advocating for equitable health care access and implementing innovative solutions to improve patient outcomes. Let us take inspiration and strive to ensure equitable health care for all.

This article was authored by Jose Lopez, MD, a cardiovascular disease fellow at the University of Miami/JFK Medical Center in Palm Beach, FL. Reach out to him using @jllbmd.
- Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure. J Am Coll Cardiol 2022;79:e263-e421.
- Gunn AH, Warraich HJ, Mentz RJ. Costs of care and financial hardship among patients with heart failure. Am Heart J 2024;269:94-107.
- Jardiance prices, coupons, copay cards & patient assistance. Drugs.com. Accessed Aug. 5, 2024. Available here.
- How much does Entresto cost per month? Drugs.com. Accessed Aug. 5, 2024. Available here.
- Gunn AH, Pendyal A. Novel cardiovascular therapeutics and the risk of financial toxicity. Nat Rev Cardiol 2024;21:349-50.
- Wang SY, Valero-Elizondo J, Ali HJ, et al. Out-of-pocket annual health expenditures and financial toxicity from healthcare costs in patients with Heart failure in the United States. J Am Heart Assoc s2021;10:e022164.
- Ali HJR, Valero-Elizondo J, Wang SY, et al. Subjective financial hardship due to medical bills among patients with heart failure in the United States: The 2014-2018 Medical Expenditure Panel Survey. J Card Fail 2022;28:1424-33.
- Aggarwal R, Vaduganathan M, Chiu N, Bhatt DL. Out-of-pocket costs for SGLT-2 (sodium-glucose transport protein-2) inhibitors in the United States. Circ Heart Fail 2022;15(3):e009099.
- Pam Beach County Project Access. Accessed Aug. 6, 2024. Available here.
- Lopez J, Latif Z, Makuvire T, DeFilippis EM. Breaking barriers. JACC Case Rep 2024;29:102354.
- Kazi DS, Wadhera RK, Rome BN. The inflation reduction act and access to high-cost cardiovascular therapies. JAMA 2023;330:1619-20.
Clinical Topics: Cardiovascular Care Team, Heart Failure and Cardiomyopathies, Prevention, Acute Heart Failure, Stress
Keywords: Cardiology Magazine, ACC Publications, Prior Authorization, Heart Failure, Medicare, Financial Stress, Insurance Coverage