PARTNER 3: Similar Echocardiographic Results With TAVR, SAVR at 5 Years
TAVR was associated with similar and stable valve hemodynamics and improved hemodynamic burden on both left and right ventricular function at five years compared with SAVR in low-risk patients with severe aortic stenosis (AS), according to a new echocardiographic analysis from PARTNER 3 published April 16 in JACC: Cardiovascular Imaging. Furthermore, among common echo parameters, only high valvulo-arterial impedance (Zva) and low rates of ventricular-to-pulmonary artery coupling (RV-PA) were associated with the primary composite endpoint of death, stroke or rehospitalization.
In the multicenter study, low-risk patients with severe AS were randomized to either SAVR (n=453) or transfemoral TAVR with the balloon-expandable SAPIEN 3 valve (n=495). Transthoracic echocardiograms were taken at baseline, 30 days and annually for five years. Among patients, 79% of both arms had echocardiograms available for this analysis.
Results showed that TAVR patients compared with SAVR patients had higher rates of mild-to-severe aortic regurgitation (24.5% vs. 6.3%, p<0.001), as well as a higher mean transaortic gradient (12.8 vs. 11.7 mm Hg, p<0.001), stroke volume index (SVI) (44.6 vs. 41.1, p<0.0001) and aortic valve area (1.87 vs. 1.82, p=0.895). In addition, low-flow SVI and left ventricular hemodynamic burden were less common with TAVR, while tricuspid annular plane systolic excursion (TAPSE) was lower and RV-PA coupling was higher.
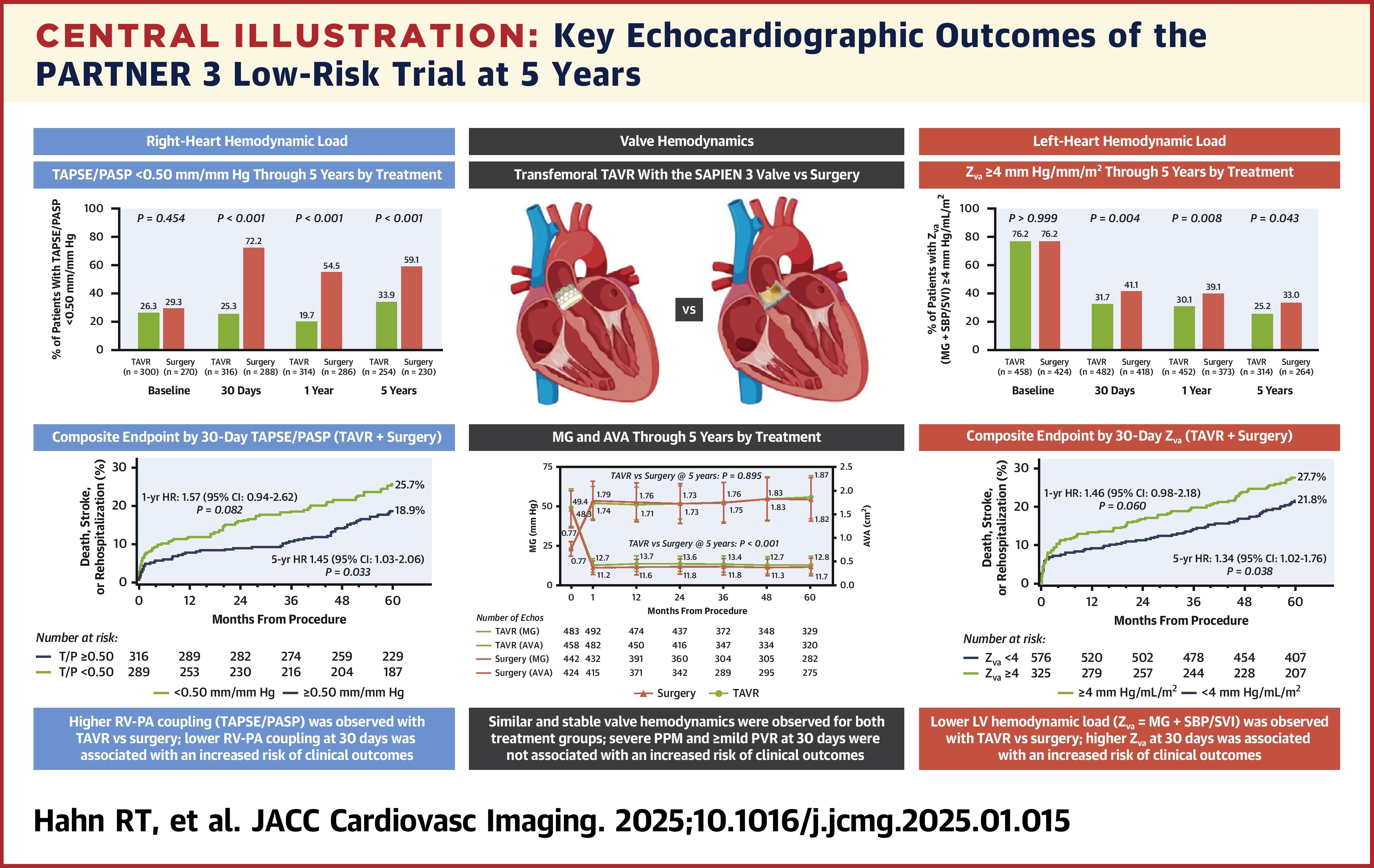
Of note, 33.0% of SAVR patients had Zva ≥4 mm Hg/mL/m2 compared with 25.2% of TAVR patients (p<0.01). Rates of RV-PA uncoupling – when TAPSE/PASP is <0.50 mm/mm Hg – were 59.1% among SAVR patients and 33.9% among TAVR patients (p<0.0001).
In both treatment groups, RV-PA uncoupling and high Zva at 30 days were the only two measured echo parameters associated with an increased risk of the primary endpoint at five years. On the other hand, 30-day moderate to severe prosthesis-patient mismatch, mild-to-severe aortic regurgitation and stroke volume index had no association.
"Our results contribute to the published reports suggesting that RV-PA coupling using TAPSE/PASP may be an important measure of outcomes in low-risk patients undergoing intervention," write study authors Rebecca T. Hahn, MD, FACC, et al. "Given these findings, it is possible that a high Zva or low TAPSE/PASP seen at 30 days warrants closer follow-up and possible improvement in medical management. Better blood pressure control or aggressive management of comorbidities could potentially improve Zva, but this requires further study."
The authors note that, due to a well-defined patient population, results might not be generalizable to larger populations or applicable to other transcatheter valve systems. Additionally, they recommend longer-term echocardiographic follow-up to continue observing the effects of TAVR beyond five years. Follow-up for the PARTNER 3 trial is planned at 10 years.
Clinical Topics: Cardiac Surgery, Invasive Cardiovascular Angiography and Intervention, Noninvasive Imaging, Valvular Heart Disease, Aortic Surgery, Cardiac Surgery and VHD, Interventions and Imaging, Interventions and Structural Heart Disease, Echocardiography/Ultrasound
Keywords: Aortic Valve Stenosis, Transcatheter Aortic Valve Replacement, Hemodynamics, Echocardiography
< Back to Listings