SWEDEHEART Registry: Early Ezetimibe Combination Therapy May Reduce CV Risk Post MI
Myocardial infarction (MI) care pathways should implement early combination therapy with statins plus ezetimibe as standard care, according to findings from an observational study published April 14 in JACC. Delaying use of combination lipid-lowering therapy (LLT) or high-intensity statin monotherapy is associated with avoidable harm.
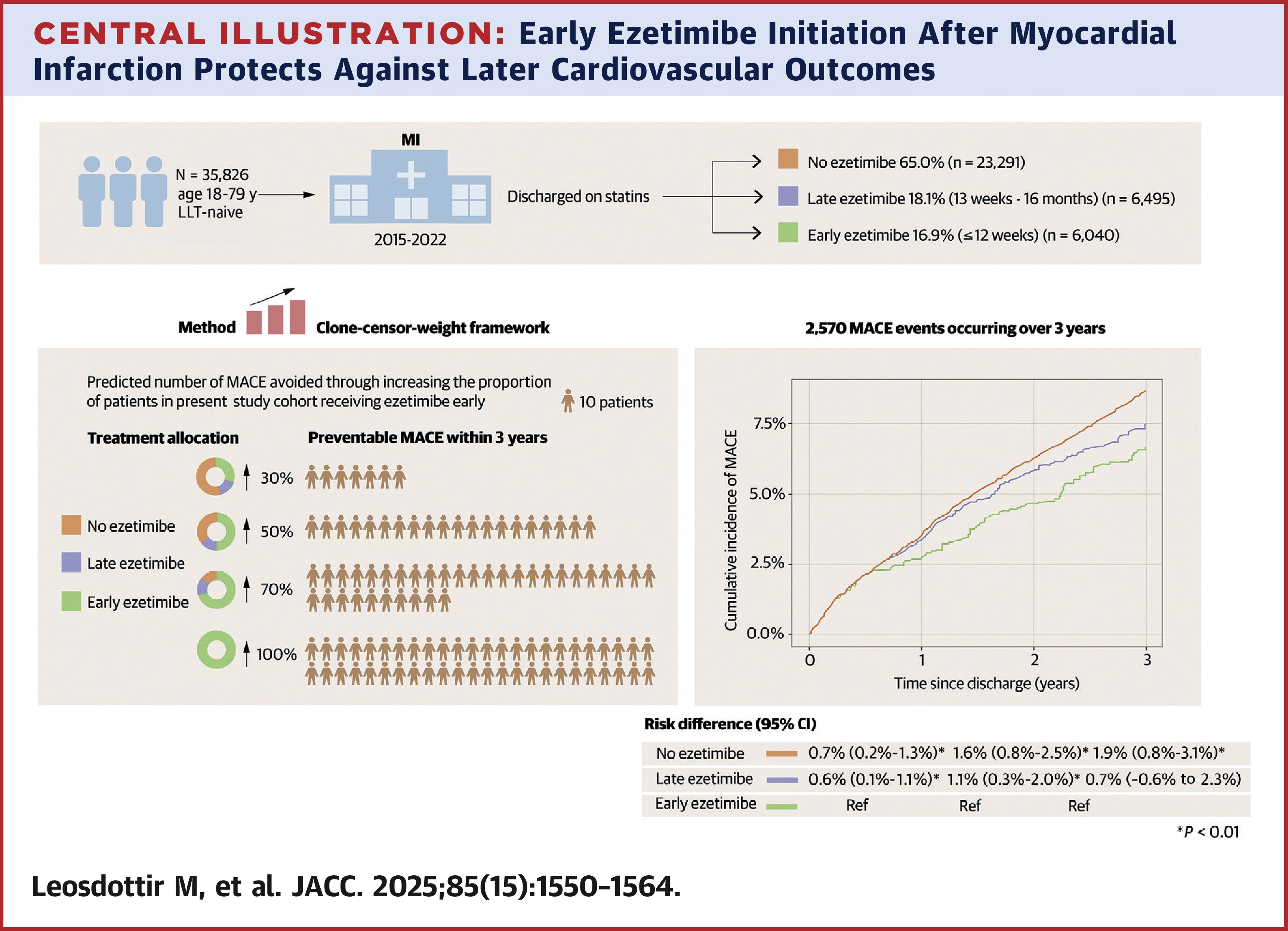
Margret Leosdottir, MD, PhD, et al., examined outcomes in 35,826 LLT-naïve patients diagnosed with a MI between 2015 and 2022 who received early (combination therapy within 12 weeks of discharge, n=6,040), late combination therapy (from 13 weeks to ≤16 weeks after discharge, n=6,495) or no ezetimibe at 16 weeks (n=23,291). Nearly all patients (98%) were taking a high-intensity statin. Their median age was 65 years and 26% were women.
Results showed that over the nearly four years of follow up, 2,570 patients experienced a major adverse cardiovascular event (MACE), including 440 cardiovascular deaths. In the early, late and no ezetimibe arms, respectively, the incidence of MACE at one year was 1.79, 2.58 and 4.03 per 100 patient-years.
Additionally, compared with early combination therapy, the weighted risk difference in MACE with late combination therapy was 0.6% at one year, 1.1% at two years and 0.7 years at three years, with a hazard ratio (HR) of 1.14 at three years. In the no ezetimibe arm, the risk difference was 0.7%, 1.6% and 1.9%, respectively, with a HR of 1.29 at three years. For cardiovascular death, the HRs were 1.64 and 1.83 in the late combination and no ezetimibe arms.
The authors write that adding ezetimibe to LLT, either early or late, led to a greater proportion of patients achieving an LDL-C of <55 mg/dL. Early, vs, late, combination therapy was associated with greater absolute and relative benefits in terms of MACE, and the approximately two-thirds of patients in the no ezetimibe arm experienced the highest risk of MACE and cardiovascular death.
"The need for combination therapy is inevitable for most patients after an MI," write Leosdottir and colleagues. "Care pathways can be streamlined with tangible health benefits if the standard of care for LLT after an MI consists of an early combination of high intensity statins with ezetimibe," they write.
In an accompanying editorial comment, Clara Chow, MBBS, PhD; Oliver Archer, MD; and Leonard Kritharides, MBBS, PhD, FACC, write, "Based on the evidence provided in the study and the culmination of evidence to date related to the topic, it seems reasonable and pragmatic to initiate combination [LLT] early in MI patients, perhaps before hospital discharge. It is also relevant to note that moderate-intensity statin in combination with ezetimibe is at least noninferior to high-intensity statin."
Clinical Topics: Dyslipidemia, Lipid Metabolism, Nonstatins, Statins
Keywords: Myocardial Infarction, Registries, Cholesterol, LDL, Ezetimibe
< Back to Listings