ACC, AHA Release New Clinical Guideline For Managing Dyslipidemia
The new ACC/AHA Guideline on the Management of Dyslipidemia offers a comprehensive “one-stop shop” for addressing the evaluation, management and monitoring of individuals with dyslipidemias, including high blood cholesterol, hypertriglyceridemia, and elevated lipoprotein(a) (Lp[a]). The document consolidates evidence-based recommendations for managing dyslipidemias and retires and replaces the 2018 Guideline on the Management of Blood Cholesterol. Read the full guideline in JACC.
Early Intervention and PREVENT Equations
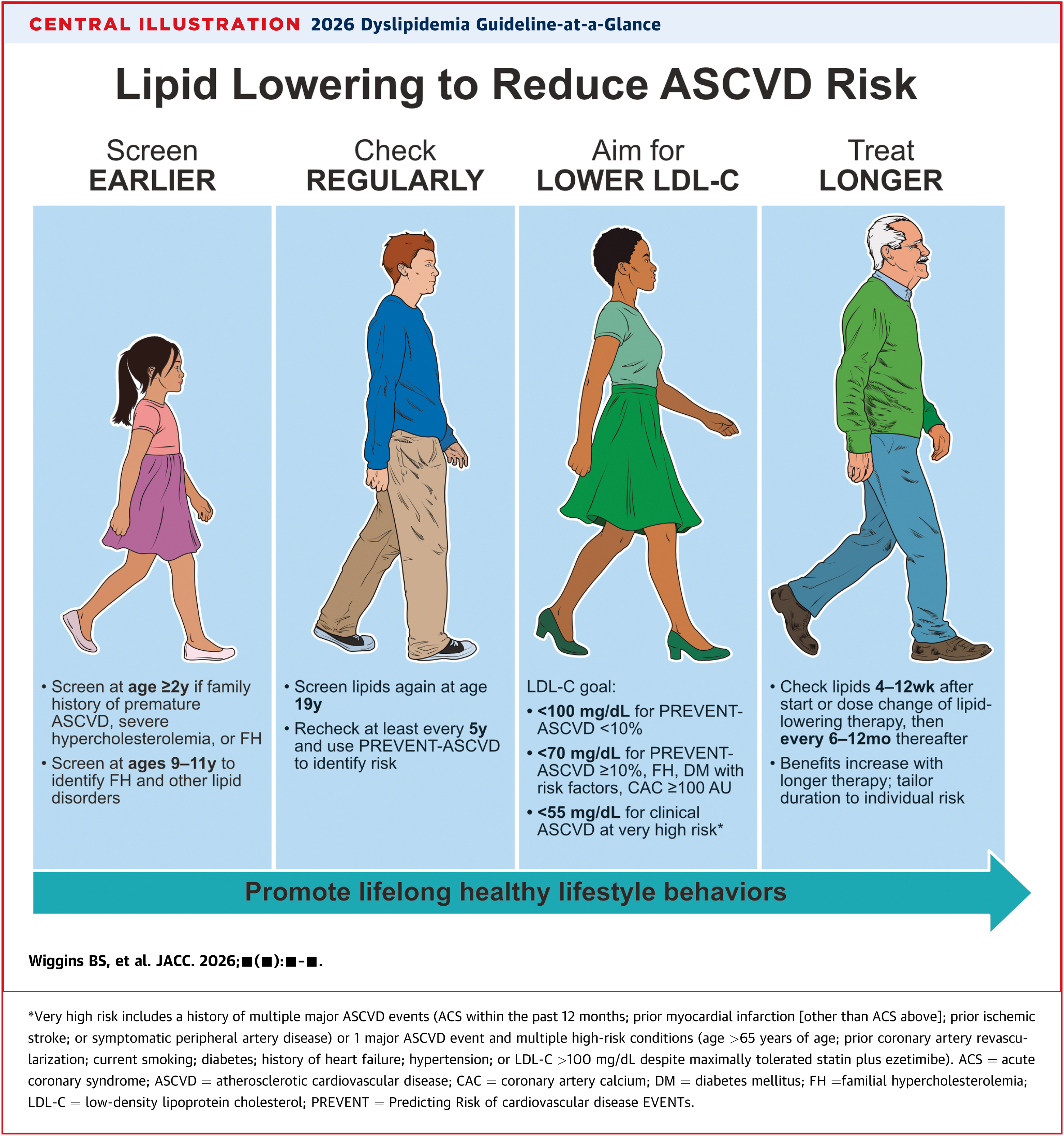
A major focus of the guideline is earlier intervention through healthy lifestyle changes, starting in childhood. Early consideration of pharmacotherapy in youth with familial hypercholesterolemia (FH) and in young adults with LDL cholesterol (LDL-C) ≥160 mg/dL or a strong family history of premature atherosclerotic cardiovascular disease (ASCVD) is also recommended.
In addition to lifestyle changes, use of the newer PREVENT-ASCVD equations instead of the older Pooled Cohort Equations for 10- and 30-year risk assessment is also recommended to guide lipid-lowering therapy (LLT) in primary prevention in adults aged 30 to 79 years. According to the guideline, LDL-lowering therapy is reasonable in adults for primary prevention of ASCVD with a borderline 10-year PREVENT-ASCVD risk estimate of 3% to <5% and is recommended for those with an intermediate 10-year PREVENT ASCVD risk of 5% to <10% following a clinician-patient discussion.
“While we want to try to optimize healthy lifestyle habits as the first step to lower cholesterol, we realize that if lipid numbers aren’t within the desirable range after a period of lifestyle optimization, we should consider adding lipid-lowering medication earlier than we would have considered 10 years ago,” said Roger S. Blumenthal, MD, FACC, chair of the guideline writing committee. “Lower [LDL-C] for longer, just like lower blood pressure for longer, results in much greater protection against future heart attack and stroke risk.”
Treatment Goals Are Back
LDL-C and non-HDL cholesterol (non-HDL-C) treatment goals are back to guide LLT, according to the guideline authors. The guideline recommends an LDL-C goal of <100 mg/dL for those at borderline or intermediate risk and <70 mg/dL in those at high risk. For individuals with ASCVD who are at very high risk of ASCVD events, the LDL-C goal should be <55 mg/dL for secondary prevention of cardiac events.
“In general, lower LDL is better, especially for people at increased risk for a heart attack or stroke,” said Pamela B. Morris, MD, FACC, vice-chair of the guideline writing committee. “Clinical trials have clearly demonstrated significant benefits for reduction in cardiovascular events when LDL-C levels are even lower than recommended in previous guidelines.”
Additional Testing
The new guideline recommends the consideration of additional tests, when appropriate, to improve cardiovascular risk assessment and assess if more intensified LDL-C lowering and management of other risk factors is needed. These include:
- Selective use of a noncontrast coronary artery calcium (CAC) scan is recommended for men over the age of 40 and women over the age of 45 with borderline or intermediate 10-year risk of heart attack or stroke. Having any amount of CAC supports an LDL-C goal of <100 mg/dL – with lower LDL-C target levels with higher amounts of calcium.
- Lp(a) should be measured at least once in adulthood. According to the guideline, lifestyle changes minimally affect Lp(a) levels, so repeat testing is generally not needed.
- Measuring Apolipoprotein B (apoB) may be used to assess any residual ASCVD risk and guide treatment among people with cardiovascular-kidney-metabolic syndrome, type 2 diabetes, high triglycerides or known cardiovascular disease who have reached their LDL-C and non-HDL-C goals. ApoB may be a more accurate risk marker than LDL-C in these groups of people.
Nonstatin Therapies and Special Considerations
If LDL-C levels are not adequately lowered by lifestyle behaviors and statin therapy, the guideline recommends the addition of nonstatin therapies. Depending upon the level of risk and patient characteristics, evidence-based options include ezetimibe and/or bempedoic acid or a PCSK9 monoclonal antibody, an injectable therapy. Inclisiran is still being studied in clinical trials to determine whether the associated LDL-C lowering translates into better outcomes and fewer cardiac events.
Special considerations are also recommended to optimize lipid management in certain adults at increased risk of heart disease. For example:
- Initiating LLT for people age 40 or older who have chronic kidney disease (stage 3 or higher), HIV or type 1 or type 2 diabetes.
- Continuing LLT in people being treated for cancer, unless contraindicated.
- Deferring most LLTs during conception, pregnancy and lactation.
In patients with persistently elevated triglycerides (TG), statin therapy remains the foundation of pharmacotherapy as an adjunct to lifestyle intervention to reduce ASCVD risk. Treatment for prevention of pancreatitis may also include TG-lowering therapies, especially in individuals with TG levels ≥1,000 mg/dL (11.3 mmol/L).
The Impact of VESALIUS
In a related Editorial Comment, Blumenthal and Morris use the recent publication of VESALIUS-CV results late last year as an example of scientific discovery outpacing the guideline development and publication timeline, noting that the VESALIUS findings “have important implications” for the prevention of ASCVD events and should be addressed in future guideline updates.
“The significant cardiovascular benefits with more intensive lowering of LDL-C to <55 mg/dL in patients without previous MI or stroke in VESALIUS-CV now blur the distinction between ASCVD risk categories when defining a ‘goal’ LDL-C value,” they write. “Thus, future updates to the 2026 ACC/AHA Dyslipidemia Guideline should include a single pathway of care for all patients with ASCVD … with an optimal LDL-C goal of <55 mg/dL to be achieved via pharmacotherapy as well as lifestyle optimization.”
Additionally, they write that “future guideline revisions should include an evidence-based recommendation for more intensive LDL-C lowering” in patients with high-risk diabetes and at least one additional high-risk feature.
The new guideline was developed in collaboration with and is endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation, Association of Black Cardiologists, American College of Preventive Medicine, American Diabetes Association, American Geriatrics Society, American Pharmacists Association, American Society for Preventive Cardiology, National Lipid Association and Preventive Cardiovascular Nurses Association.
Clinical Topics: Diabetes and Cardiometabolic Disease, Dyslipidemia, Prevention, Hypertriglyceridemia, Lipid Metabolism, Nonstatins, Novel Agents, Primary Hyperlipidemia, Statins
Keywords: PCSK9 protein, human, Blood Pressure, Calcium, Cholesterol, LDL, Diabetes Mellitus, Type 2, Hydroxymethylglutaryl-CoA Reductase Inhibitors, Proprotein Convertase 9, Secondary Prevention, Neoplasms, Hyperlipoproteinemia Type II, Renal Insufficiency, Chronic, Hypertriglyceridemia, Antibodies, Monoclonal, Primary Prevention, Apolipoproteins, Dyslipidemias, Myocardial Infarction, Triglycerides, Kidney, Stroke
< Back to Listings