New ACC Concise Clinical Guidance Report ‘Weighs In’ on Medical Weight Management For Optimizing CV Health
Given the varying causes of obesity and the wide range of physiological consequences with direct effects on cardiovascular risk factors, the ACC's newest Concise Clinical Guidance (CCG) report provides a framework for clinicians to medically manage obesity using the "ever-expanding set of tools to assist patients in diagnosis, weight reduction, and CVD risk mitigation."
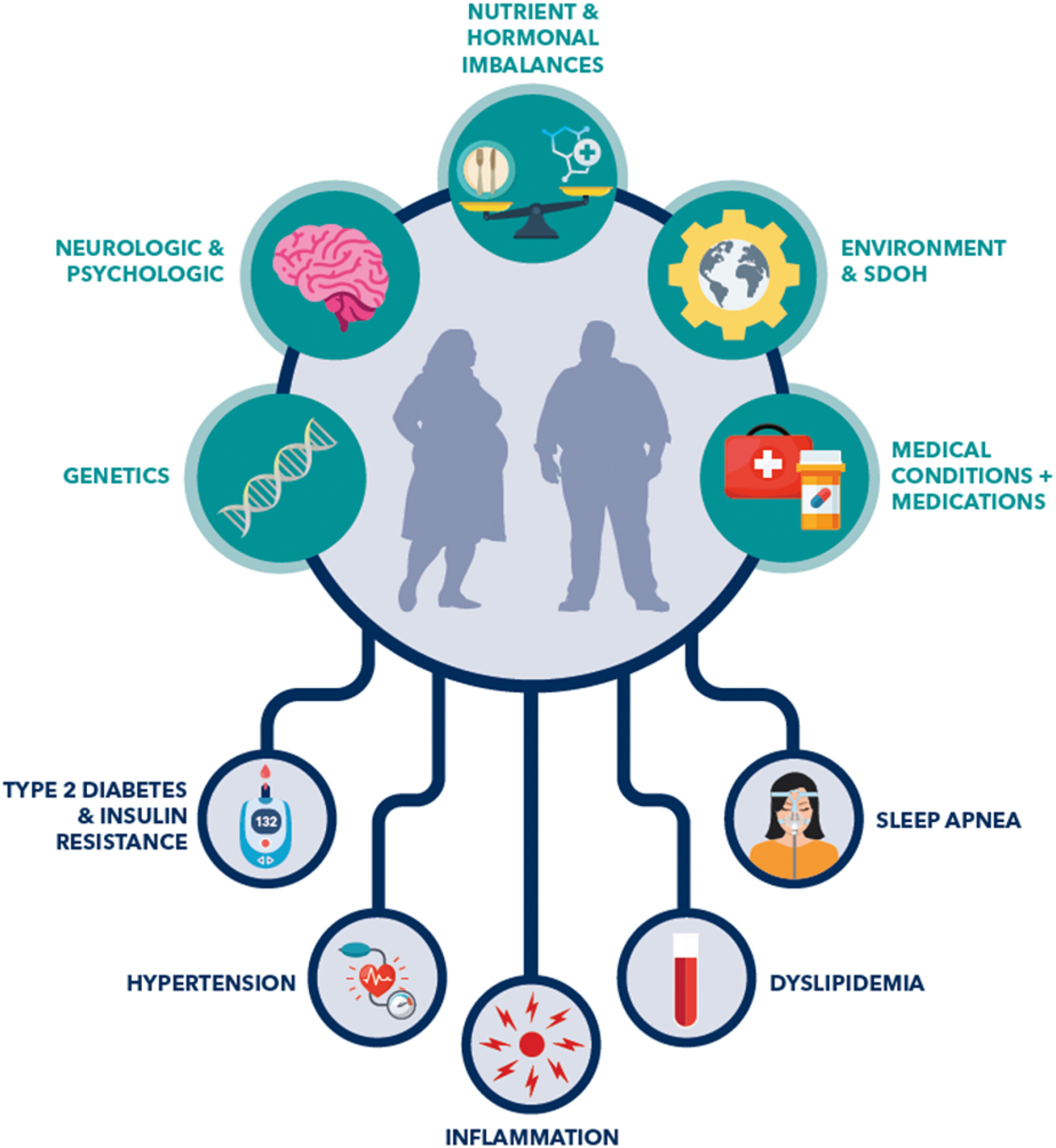
The CCG, led by Chair Olivia Gilbert, MD, MSc, FACC, and Vice Chair Martha Gulati, MD, MS, FACC, and published in JACC, highlights the multiple causes of obesity, including genetic, neurological and psychological factors, as well as nutrient and hormonal imbalances, environmental and social determinants of health, and medical conditions and medications. It also discusses obesity-related cardiovascular disease risks like sleep apnea, dyslipidemia, inflammation, hypertension and type 2 diabetes, which can increasingly be addressed with modern obesity medications with fewer risks than procedure-based interventions.
Importantly, the CCG also outlines the clinical decision-making process for clinicians to incorporate these and future pharmacologic weight management strategies into cardiovascular care, highlighting the following key areas:
- Rationale and Eligibility – Pharmacotherapy strikes the balance between effectiveness and invasiveness. Eligibility may be determined by BMI thresholds or other risk indicators. These therapies can be adjusted to minimize adverse effects and personalize care.
- Pharmacological Options – Among U.S. Food and Drug Administration-approved medications, the GLP-1 receptor agonist semaglutide and the GLP-1/GIP receptor agonist tirzepatide have demonstrated the highest efficacy. Clinical trial and real-world observational data support slightly greater weight loss with tirzepatide. Insurance coverage, availability and affordability are likely to dictate agent selection.
- Impact on Cardiovascular Risk – Clinical evidence supports medications leading to a reduction in major adverse cardiovascular events – including cardiovascular death, myocardial infarction and stroke – particularly in individuals with type 2 diabetes and elevated cardiovascular risk.
- Multidisciplinary Care Approaches – Team-based approaches are critical for effective weight management, helping to assess modifiable risk factors, identify comorbidities and tailor treatment strategies.
- Reducing Bias and Improving Experience – Clinicians should make every effort to validate the lifelong journey that patients experience with this chronic disease, placing emphasis on person-first language, creating welcoming clinical environments and addressing weight stigmas.
- Access Considerations – Lack of insurance coverage remains a major barrier for patients. Initial strategies to improve access to therapies include identifying individuals most likely to benefit, close monitoring of treatment outcomes and price negotiations.
"Patients should not be required to 'try and fail' lifestyle changes prior to initiating pharmacotherapy; nonetheless, lifestyle interventions should always be offered in conjunction with obesity medications," said Gilbert. "Weight management by the cardiovascular community needs to be embraced, given both the prevalence of obesity and the impact it has on many forms of [cardiovascular disease]."
The new CCG follows on the heels of the College's first-ever Scientific Statement addressing the management of obesity specifically in adults with heart failure (HF), with a specific focus on those with stage 2 HF with preserved ejection fraction (HFpEF). Read the statement.
Keywords: Glucagon-Like Peptide 1, Weight Loss, Semaglutide, Obesity
< Back to Listings